
Abstract
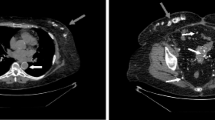
Bisphosphonates are the mainstay treatment for postmenopausal osteoporosis. Although bisphosphonates are safety drugs, they have numerous side-effects such as arthralgia, elevated erythrocyte sedimentation rate and C-reactive protein, gastrointestinal disturbances, and flu-like illness with symptoms of fatigue, fever, chills, malaise, and myalgia. We present a case of acute polyarthritis after administration of alendronate and risedronate in a 52-year-old woman. To the best of the author’s knowledge, this is the first case of acute polyarthritis induced by per os administration of both alendronate and risedronate during weekly usage. This is a report of a 52-year-old woman admitted to our hospital every week in a month, within 48 h, after receiving three times alendronate and one time risedronate with diffuse arthralgias, miyalgias, and swelling with effusions in both wrists, both ankles, interphalangeal joints in both hands and feet, and in both knees. When we discontinued alendronate and risedronate, oral raloxifene (60 mg/day) with oral calcium (1 g/day), and vitamin D3 (800 IU/day) was initiated. The symptoms regressed in 1 week. During the 1 year follow-up period, no myalgia, arthritis, or synovitis was detected. The side-effects of bisphosphonates are rarely reported in the literature. We believe that the prevalance of these side-effects would increase by closer follow-up of patients receiving these medications. To our knowledge, this patient is the first reported case of acute polyarthritis induced by per os administration of both alendronate and risedronate during weekly usage.

Similar content being viewed by others

References
Yemisci OU, Yalbuzdag SA, Karatas M (2010) Risedronate-induced arthritis. J Clin Rheumatol 16:168–169
Gwynne Jones DP, Savage RL, Highton J (2008) Alendronate-induced synovitis. J Rheumatol 35:537–538
Reginster JY, Adami S, Lakatos P et al (2006) Efficacy and tolerability of once-monthly oral ibandronate in postmenopausal osteoporosis: 2 year results from the MOBILE study. Ann Rheum Dis 65:654–661
Diaz-Borjon A, Seyler TM, Chen NL, Lim SS (2006) Bisphosphonate-associated arthritis. J Clin Rheumatol 12:131–133
Miller PD, Recker RR, Reginster JY (2012) Efficacy of monthly oral ibandronate is sustained over 5 years: the MOBILE long-term extension study. Osteoporos Int 23:1747–1756
Thompson K, Rogers MJ (2004) Statins prevent bisphosphonate-induced gamma, delta-T-cell proliferation and activation in vitro. J Bone Miner Res 19:278–288
Benford HL, Frith JC, Auriola S, Mönkkönen J, Rogers MJ (1999) Farnesol and geranylgeraniol prevent activation of caspases by aminobisphosphonates: biochemical evidence for two distinct pharmacological classes of bisphosphonate drugs. Mol Pharmacol 56:131–140
Gerster JH (2004) Acute polyarthritis related to once-weekly alendronate in a woman with osteoporosis. J Rheumatol 31:829–830
Frederiksen L, Junker P, Brixen KT (2007) Persistent polyarticular synovitis after treatment with alendronate. Ugeskr Laeger 169:1583–1584
Gökkus K, Yazicioglu G, Sagtas E, Uyan A, Aydin AT (2016) Possible alendronate-induced polyarticular synovitis. J Postgrad Med 62:126–128
Jones DG, Savage R, Highton J (2005) Synovitis induced by alendronic acid can present as acute carpal tunnel syndrome. BMJ 330:74
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
None.
Rights and permissions
About this article

Cite this article
Uğurlar, M. Alendronate- and risedronate-induced acute polyarthritis. Osteoporos Int 27, 3383–3385 (2016). https://doi.org/10.1007/s00198-016-3695-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-016-3695-3