
Abstract
Summary
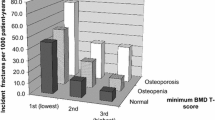
In this study, the area under the curve was highest when using the lowest vertebral body T-score to diagnose osteoporosis. In men for whom hip imaging is not possible, the lowest vertebral body T-score improves the ability to diagnose osteoporosis in men who are likely to have an incident fragility fracture.
Introduction
Spine T-scores have limited ability to predict fragility fracture. We hypothesized that using lowest vertebral body T-score to diagnose osteoporosis would better predict fracture.
Methods
Among men enrolled in the Osteoporotic Fractures in Men Study, we identified cases with incident clinical fracture (n = 484) and controls without fracture (n = 1,516). We analyzed the lumbar spine bone mineral density (BMD) in cases and controls (n = 2,000) to record the L1–L4 (referent), the lowest vertebral body, and International Society for Clinical Densitometry (ISCD)-determined T-scores using a male normative database and the L1–L4 T-score using a female normative database. We compared the ability of method to diagnose osteoporosis and, therefore, to predict incident clinical fragility fracture, using area under the receiver operator curves (AUCs) and the net reclassification index (NCI) as measures of diagnostic accuracy. ISCD-determined T-scores were determined in only 60 % of participants (n = 1,205).
Results
Among 1,205 men, the AUC to predict incident clinical fracture was 0.546 for L1–L4 male, 0.542 for the L1–L4 female, 0.585 for lowest vertebral body, and 0.559 for ISCD-determined T-score. The lowest vertebral body AUC was the only method significantly different from the referent method (p = 0.002). Likewise, a diagnosis of osteoporosis based on the lowest vertebral body T-score demonstrated a significantly better net reclassification index (NRI) than the referent method (net NRI +0.077, p = 0.005). By contrast, the net NRI for other methods of analysis did not differ from the referent method.
Conclusion
Our study suggests that in men, the lowest vertebral body T-score is an acceptable method by which to estimate fracture risk.


Similar content being viewed by others


References
Cummings SR, Black DM, Nevitt MC, Browner W, Cauley J, Ensrud K, Genant HK, Palermo L, Scott J, Vogt TM (1993) Bone density at various sites for prediction of hip fractures. The Study of Osteoporotic Fractures Research Group. Lancet 341(8837):72–75
Melton LJ 3rd, Atkinson EJ, O’Connor MK, O'Fallon WM, Riggs BL (1998) Bone density and fracture risk in men. J Bone Miner Res 13(12):1915–1923
Cummings SR, Cawthon PM, Ensrud KE, Cauley JA, Fink HA, Orwoll ES (2006) BMD and risk of hip and nonvertebral fractures in older men: a prospective study and comparison with older women. J Bone Miner Res 21(10):1550–1556. doi:10.1359/jbmr.060708
Liu G, Peacock M, Eilam O, Dorulla G, Braunstein E, Johnston CC (1997) Effect of osteoarthritis in the lumbar spine and hip on bone mineral density and diagnosis of osteoporosis in elderly men and women. Osteoporos Int 7(6):564–569
Genant HK, Engelke K, Fuerst T, Gluer CC, Grampp S, Harris ST, Jergas M, Lang T, Lu Y, Majumdar S, Mathur A, Takada M (1996) Noninvasive assessment of bone mineral and structure: state of the art. J Bone Miner Res 11(6):707–730
Hamdy RC, Petak SM, Lenchik L (2002) Which central dual X-ray absorptiometry skeletal sites and regions of interest should be used to determine the diagnosis of osteoporosis? J Clin Densitom 5(Suppl):S11–S18
Hansen KE, Binkley N, Christian R, Vallarta-Ast N, Krueger D, Drezner MK, Blank RD (2005) Interobserver reproducibility of criteria for vertebral body exclusion. J Bone Miner Res 20(3):501–508
Tsang JF, Leslie WD (2007) Exclusion of focal vertebral artifacts from spine bone densitometry and fracture prediction: a comparison of expert physicians, three computer algorithms, and the minimum vertebra. J Bone Miner Res 22(6):789–798. doi:10.1359/jbmr.070319
Vokes TJ, Gillen DL, Lovett J, Favus MJ (2005) Comparison of T-scores from different skeletal sites in differentiating postmenopausal women with and without prevalent vertebral fractures. J Clin Densitom 8(2):206–215
Hansen KE, Vallarta-Ast N, Krueger D, Gangnon R, Drezner MK, Binkley N (2005) Use of the lowest lumbar vertebral body T-score to diagnose lumbar osteoporosis in men: is “cherry picking” appropriate? J Clin Densitom 7(4):376–381
Orwoll E, Blank JB, Barrett-Connor E, Cauley J, Cummings S, Ensrud K, Lewis C, Cawthon PM, Marcus R, Marshall LM, McGowan J, Phipps K, Sherman S, Stefanick ML, Stone K (2005) Design and baseline characteristics of the osteoporotic fractures in men (MrOS) study—a large observational study of the determinants of fracture in older men. Contemp Clin Trials 26(5):569–585
Blank JB, Cawthon PM, Carrion-Petersen ML, Harper L, Johnson JP, Mitson E, Delay RR (2005) Overview of recruitment for the osteoporotic fractures in men study (MrOS). Contemp Clin Trials 26(5):557–568. doi:10.1016/j.cct.2005.05.005
(2005) ISCD Official Positions of the International Society for Clinical Densitometry. In: ISCD Position Development Conference, Vancouver, BC, Canada, 2005
Kerr KF, Wang Z, Janes H, McClelland RL, Psaty BM, Pepe MS (2014) Net reclassification indices for evaluating risk prediction instruments: a critical review. Epidemiology 25(1):114–121. doi:10.1097/EDE.0000000000000018
Fink HA, Harrison SL, Taylor BC, Cummings SR, Schousboe JT, Kuskowski MA, Stone KL, Ensrud KE (2008) Differences in site-specific fracture risk among older women with discordant results for osteoporosis at hip and spine: study of osteoporotic fractures. J Clin Densitom 11(2):250–259. doi:10.1016/j.jocd.2007.12.018
Chen P, Miller PD, Binkley NC, Kendler DL, Wong M, Krohn K (2008) Use of lowest single lumbar spine vertebra bone mineral density T-score and other T-score approaches for diagnosing osteoporosis and relationships with vertebral fracture status. J Clin Densitom 11(4):525–531. doi:10.1016/j.jocd.2008.04.009
Acknowledgments
We thank the National Osteoporosis Foundation for grant support for the substudy. The Osteoporotic Fractures in Men (MrOS) Study is supported by National Institutes of Health funding. The following institutes provide support: the National Institute of Arthritis and Musculoskeletal and Skin Diseases (NIAMS), the National Institute on Aging (NIA), the National Center for Research Resources (NCRR), and NIH Roadmap for Medical Research under the following grant numbers: U01 AR45580, U01 AR45614, U01 AR45632, U01 AR45647, U01 AR45654, U01 AR45583, U01 AG18197, U01-AG027810, and UL1 TR000128.
Conflicts of interest
Karen E. Hansen is a consultant to Takeda Pharmaceuticals and Deltanoid Pharmaceuticals. Eric Orwoll is a consultant to Amgen, Merck, and Lilly and receives research support from Amgen, Merck, and Lilly. Robert D. Blank, Lisa Palermo, and Howard Fink report no conflicts of interest.
Author information
Authors and Affiliations
Consortia
Corresponding author
Rights and permissions
About this article

Cite this article
Hansen, K.E., Blank, R.D., Palermo, L. et al. What analytic method should clinicians use to derive spine T-scores and predict incident fractures in men? Results from the MrOS study. Osteoporos Int 25, 2181–2188 (2014). https://doi.org/10.1007/s00198-014-2744-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-014-2744-z