
Abstract
Summary
This study for the first time investigates the association of bone mineral density (BMD) with angiographically determined coronary atherosclerosis in men. Our data show that the prevalence of low BMD is very high in men undergoing coronary angiography. However, neither osteopenia nor osteoporosis is associated with an increased prevalence of angiographically determined coronary atherosclerosis.
Introduction
The association of low BMD with angiographically determined coronary atherosclerosis in men is unknown.
Methods
We enrolled 623 consecutive men undergoing coronary angiography for the evaluation of established or suspected coronary artery disease (CAD). BMD was assessed by dual X-ray absorptiometry. CAD was diagnosed in the presence of any coronary artery lumen narrowing at angiography; coronary stenoses with lumen narrowing ≥50% were considered significant.
Results
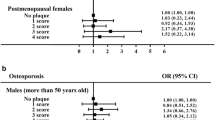
From the total study cohort (mean age of 64 ± 11 years), 207 patients (33.2%) had osteopenia and 65 (10.4%) had osteoporosis; at angiography, CAD was diagnosed in 558 patients (89.6%) and 403 (64.7%) had significant coronary stenoses. In multivariate logistic regression analysis neither osteopenia nor osteoporosis was associated with an increased prevalence of CAD (adjusted odds ratios (ORs) = 0.71 [95% confidence interval 0.40–1.23]; p = 0.222 and 1.03 [0.38–2.80]; p = 0.955, respectively) or with significant coronary stenoses (OR 0.74 [0.52–1.07], p = 0.112 and 0.72 [0.41–1.26]; p = 0.251, respectively). Also, as a continuous variable, BMD was not associated with angiographically diagnosed CAD.
Conclusions
The prevalence of low BMD is very high in men undergoing coronary angiography. However, low BMD is not associated with angiographically determined coronary atherosclerosis in men.

Similar content being viewed by others


References
Epstein FH (1996) Cardiovascular disease epidemiology: a journey from the past into the future. Circulation 93:1755–1764
Cooper C, Atkinson EJ, Jacobsen SJ et al (1993) Population-based study of survival after osteoporotic fractures. Am J Epidemiol 137:1001–1005
Keene GS, Parker MJ, Pryor GA (1993) Mortality and morbidity after hip fractures. BMJ 307:1248–1250
Burge R, Dawson-Hughes B, Solomon DH et al (2007) Incidence and economic burden of osteoporosis-related fractures in the United States, 2005–2025. J Bone Miner Res 22:465–475
Dolan P, Torgerson DJ (1998) The cost of treating osteoporotic fractures in the United Kingdom female population. Osteoporos Int 8:611–617
Cooper C (1997) The crippling consequences of fractures and their impact on quality of life. Am J Med 103:12S–17S
Peterson AM, McGhan WF (2005) Pharmacoeconomic impact of non-compliance with statins. Pharmacoeconomics 23:13–25
van Jaarsveld CH, Sanderman R, Ranchor AV et al (2002) Gender-specific changes in quality of life following cardiovascular disease: a prospective study. J Clin Epidemiol 55:1105–1112
Tanko LB, Bagger YZ, Christiansen C (2003) Low bone mineral density in the hip as a marker of advanced atherosclerosis in elderly women. Calcif Tissue Int 73:15–20
Barengolts EI, Berman M, Kukreja SC et al (1998) Osteoporosis and coronary atherosclerosis in asymptomatic postmenopausal women. Calcif Tissue Int 62:209–213
Kiel DP, Kauppila LI, Cupples LA et al (2001) Bone loss and the progression of abdominal aortic calcification over a 25 year period: the Framingham Heart Study. Calcif Tissue Int 68:271–276
Hak AE, Pols HA, van Hemert AM et al (2000) Progression of aortic calcification is associated with metacarpal bone loss during menopause: a population-based longitudinal study. Arterioscler Thromb Vasc Biol 20:1926–1931
Hofbauer LC, Brueck CC, Shanahan CM et al (2007) Vascular calcification and osteoporosis—from clinical observation towards molecular understanding. Osteoporos Int 18:251–259
Doherty TM, Detrano RC (1994) Coronary arterial calcification as an active process: a new perspective on an old problem. Calcif Tissue Int 54:224–230
Schmid K, McSharry WO, Pameijer CH, Binette JP (1980) Chemical and physicochemical studies on the mineral deposits of the human atherosclerotic aorta. Atherosclerosis 37:199–210
Shanahan CM, Cary NR, Metcalfe JC, Weissberg PL (1994) High expression of genes for calcification-regulating proteins in human atherosclerotic plaques. J Clin Invest 93:2393–2402
Bostrom K, Watson KE, Horn S et al (1993) Bone morphogenetic protein expression in human atherosclerotic lesions. J Clin Invest 91:1800–1809
Giachelli CM, Bae N, Almeida M et al (1993) Osteopontin is elevated during neointima formation in rat arteries and is a novel component of human atherosclerotic plaques. J Clin Invest 92:1686–1696
Dhore CR, Cleutjens JP, Lutgens E et al (2001) Differential expression of bone matrix regulatory proteins in human atherosclerotic plaques. Arterioscler Thromb Vasc Biol 21:1998–2003
Von der RP, Hansen MA, Hassager C (1999) The association between low bone mass at the menopause and cardiovascular mortality. Am J Med 106:273–278
Samelson EJ, Kiel DP, Broe KE et al (2004) Metacarpal cortical area and risk of coronary heart disease: the Framingham Study. Am J Epidemiol 159:589–595
Trivedi DP, Khaw KT (2001) Bone mineral density at the hip predicts mortality in elderly men. Osteoporos Int 12:259–265
Tanko LB, Christiansen C, Cox DA et al (2005) Relationship between osteoporosis and cardiovascular disease in postmenopausal women. J Bone Miner Res 20:1912–1920
Fuster V, Badimon L, Badimon JJ, Chesebro JH (1992) The pathogenesis of coronary artery disease and the acute coronary syndromes (2). N Engl J Med 326:310–318
Fuster V, Badimon L, Badimon JJ, Chesebro JH (1992) The pathogenesis of coronary artery disease and the acute coronary syndromes (1). N Engl J Med 326:242–250
Marcovitz PA, Tran HH, Franklin BA et al (2005) Usefulness of bone mineral density to predict significant coronary artery disease. Am J Cardiol 96:1059–1063
Tekin GO, Kekilli E, Yagmur J et al (2008) Evaluation of cardiovascular risk factors and bone mineral density in post menopausal women undergoing coronary angiography. Int J Cardiol 131:66–69
Sytkowski PA, D’Agostino RB, Belanger A, Kannel WB (1996) Sex and time trends in cardiovascular disease incidence and mortality: the Framingham Heart Study, 1950–1989. Am J Epidemiol 143:338–350
Chobanian AV, Bakris GL, Black HR et al (2003) The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure: the JNC 7 report. JAMA 289:2560–2572
Alberti KG, Zimmet PZ (1998) Definition, diagnosis and classification of diabetes mellitus and its complications. Part 1: diagnosis and classification of diabetes mellitus provisional report of a WHO consultation. Diabet Med 15:539–553
Saely CH, Koch L, Schmid F et al (2006) Lipoprotein(a), type 2 diabetes and vascular risk in coronary patients. Eur J Clin Invest 36:91–97
Kanis JA, Melton LJ III, Christiansen C et al (1994) The diagnosis of osteoporosis. J Bone Miner Res 9:1137–1141
Drexel H, Aczel S, Marte T et al (2005) Is atherosclerosis in diabetes and impaired fasting glucose driven by elevated LDL cholesterol or by decreased HDL cholesterol? Diabetes Care 28:101–107
Muendlein A, Saely CH, Marte T et al (2008) Synergistic effects of the apolipoprotein E epsilon3/epsilon2/epsilon4, the cholesteryl ester transfer protein TaqIB, and the apolipoprotein C3–482 C>T polymorphisms on their association with coronary artery disease. Atherosclerosis 199:179–186
Marte T, Saely CH, Schmid F et al (2009) Effectiveness of atrial fibrillation as an independent predictor of death and coronary events in patients having coronary angiography. Am J Cardiol 103:36–40
Saely CH, Drexel H, Sourij H et al (2008) Key role of postchallenge hyperglycemia for the presence and extent of coronary atherosclerosis: an angiographic study. Atherosclerosis 199:317–322
Drexel H, Amann FW, Rentsch K et al (1992) Relation of the level of high-density lipoprotein subfractions to the presence and extent of coronary artery disease. Am J Cardiol 70:436–440
Drexel H, Amann FW, Beran J et al (1994) Plasma triglycerides and three lipoprotein cholesterol fractions are independent predictors of the extent of coronary atherosclerosis. Circulation 90:2230–2235
Gluer CC, Eastell R, Reid DM et al (2004) Association of five quantitative ultrasound devices and bone densitometry with osteoporotic vertebral fractures in a population-based sample: the OPUS Study. J Bone Miner Res 19:782–793
Haussler B, Gothe H, Gol D et al (2007) Epidemiology, treatment and costs of osteoporosis in Germany—the BoneEVA Study. Osteoporos Int 18:77–84
Ebeling PR (2008) Clinical practice. Osteoporosis in men. N Engl J Med 358:1474–1482
Hoefle G, Saely CH, Aczel S et al (2005) Impact of total and central obesity on vascular mortality in patients undergoing coronary angiography. Int J Obes (Lond) 29:785–791
Saely CH, Koch L, Schmid F et al (2006) Adult Treatment Panel III 2001 but not International Diabetes Federation 2005 criteria of the metabolic syndrome predict clinical cardiovascular events in subjects who underwent coronary angiography. Diabetes Care 29:901–907
Varma R, Aronow WS, Basis Y et al (2008) Relation of bone mineral density to frequency of coronary heart disease. Am J Cardiol 101:1103–1104
Saely CH, Vonbank A, Rein P et al (2008) Alanine aminotransferase and gamma-glutamyl transferase are associated with the metabolic syndrome but not with angiographically determined coronary atherosclerosis. Clin Chim Acta 397:82–86
Acknowledgements
The VIVIT institute thanks Dr. Egmond Frommelt and the Innovationsstiftung of the Liechtenstein Global Trust (LGT) Bank (Bendern, Liechtenstein), Dr. Karl Josef Hier, Peter Goop Stiftung (Vaduz, Liechtenstein), Gabriela Dür and the Vorarlberger Landesregierung (Bregenz, Austria), Prof. Willi A. Ribi and the University of the Principality of Liechtenstein, as well as the Fachhochschule Dornbirn (Dornbirn, Austria) for providing us with generous research grants. We are grateful to Franz Rauch and the Vorarlberger Industriellenvereinigung (Bregenz, Austria), to Dr. Peter Woess and the Vorarlberger Aerztekammer (Dornbirn, Austria), to Dr. Elmar Bechter, and to Luis Patsch, Drs. Gerald Fleisch and Till Hornung, Directors, Vorarlberger Landeskrankenhaus-Betriebsgesellschaft (Feldkirch, Austria), for continuously supporting our Research Institute. The study was part-financed by the ‘Land Vorarlberg’ and the ‘Europaeischer Fonds fuer regionale Entwicklung’ (EFRE). The sponsor did not participate in analyses or influence the decision to submit for publication.
Conflicts of interest
None.
Author information
Authors and Affiliations
Corresponding author
Additional information
This work was supported by grants from the following institutions: Innovationsstiftung of the Liechtenstein Global Trust (LGT) Bank (Bendern, Liechtenstein); Peter Goop Stiftung (Vaduz, Liechtenstein); Fachhochschule Dornbirn (Dornbirn, Austria); Institute for Clinical Chemistry at the Academic Teaching Hospital Feldkirch (Feldkirch, Austria); Vorarlberger Industriellenvereinigung (Bregenz, Austria); Vorarlberger Landesregierung (Bregenz, Austria); and Vorarlberger Landeskrankenhaus-Betriebsgesellschaft (Feldkirch, Austria).
Rights and permissions
About this article
Cite this article
Beer, S., Saely, C.H., Hoefle, G. et al. Low bone mineral density is not associated with angiographically determined coronary atherosclerosis in men. Osteoporos Int 21, 1695–1701 (2010). https://doi.org/10.1007/s00198-009-1103-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-009-1103-y