
Abstract
Summary
Using a Markov state-transition model, we estimated fractures averted with risedronate using two different types of clinical efficacy data. Summary data, as opposed to individual patient data (IPD), underestimated the number of fractures averted when applied in a specified high risk population. The choice of clinical efficacy data is an important consideration in health economic models evaluating osteoporosis therapies.
Introduction
This paper contrasts fracture reduction estimates for risedronate utilizing efficacy data from two approaches to meta-analysis: summary data versus individual patient data. We also examined differences in fracture reduction explained by varied cohort selection, especially the inclusion of low- versus high-risk populations.
Methods
Using a Markov state-transition model, we compared fractures averted over 3 years in a hypothetical cohort by inputting fracture risk reduction estimates (risedronate versus placebo) from two data sources (summary data versus IPD). The cohort consisted of 100,000 Canadian women, age ≥65 years with osteoporosis (WHO criteria T-score ≤ -2.5) and prevalent morphometric vertebral fracture.
Results
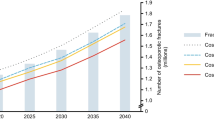
Non-vertebral fractures averted with risedronate were: 3,571 and 6,584 per 100,000 women for summary data and IPD, respectively. For vertebral fractures, the numbers were 8,552 and 10,127. When IPD versus summary data was used, an additional 3,013 more non-vertebral fractures and 1,575 vertebral fractures were averted.
Discussion
Relative risk estimates from IPD analyses were the best choice for modelling fracture outcomes when applied in a specified high-risk population. In addition to superior statistical methodology, they utilized RCT cohorts that are more representative of higher risk patients requiring treatment (osteoporotic women ≥65 years with a prevalent vertebral fracture).
Similar content being viewed by others
References
Sawka AM, Thabane L, Papaioannou A, Gafni A, Ioannidis G, Hanley DA, Papadimitropoulos E, Pickard L, Adachi JD (2004) The number of Canadian men and women needed to be screened to detect a case of osteoporosis: a population-based study from the Canadian Multicentre Osteoporosis Study (CaMos). J Bone Miner Res 19:S368
Doherty DA, Sanders KM, Kotowicz MA, Prince RL (2001) Lifetime and five-year age-specific risks of first and subsequent osteoporotic fractures in postmenopausal women. Osteoporos Int 12:16–23
Cummings SR, Black DM, Rubin SM (1989) Lifetime risks of hip, Colles', or vertebral fracture and coronary heart disease among white postmenopausal women. Arch Intern Med 149:2445–2448
Melton LJ III, Chrischilles EA, Cooper C, Lane AW, Riggs BL (1992) Perspective. How many women have osteoporosis? J Bone Miner Res 7:1005–1010
Wiktorowicz ME, Goeree R, Papaioannou A, Adachi JD, Papadimitropoulos E (2001) Economic implications of hip fracture: health service use, institutional care and cost in Canada. Osteoporos Int 12:271–278
Brown JP, Josse RG (2002) clinical practice guidelines for the diagnosis and management of osteoporosis in Canada. CMAJ 167:S1–34
Dolovich MB, Ahrens RC, Hess DR, Anderson P, Dhand R, Rau JL, Smaldone GC, Guyatt G (2005) Device selection and outcomes of aerosol therapy: evidence-based guidelines: American College of Chest Physicians/American College of Asthma, Allergy, and Immunology. Chest 127:335–371
Cranney A, Tugwell P, Adachi J, Weaver B, Zytaruk N, Papaioannou A, Robinson V, Shea B, Wells G, Guyatt G (2002) Meta-analyses of therapies for postmenopausal osteoporosis. III. Meta-analysis of risedronate for the treatment of postmenopausal osteoporosis. Endocr Rev 23:517–523
Cranney A, Wells G, Willan A, Griffith L, Zytaruk N, Robinson V, Black D, Adachi J, Shea B, Tugwell P, Guyatt G (2002) Meta-analyses of therapies for postmenopausal osteoporosis. II. Meta-analysis of alendronate for the treatment of postmenopausal women. Endocr Rev 23:508–516
Boonen S, Laan RF, Barton IP, Watts NB (2005) Effect of osteoporosis treatments on risk of non-vertebral fractures: review and meta-analysis of intention-to-treat studies. Osteoporos Int 16:1291–1298
Delmas PD Seeman E (2004) Changes in bone mineral density explain little of the reduction in vertebral or nonvertebral fracture risk with anti-resorptive therapy. Bone 34:599–604
Adachi JD, Rizzoli R, Boonen S Li Z, Meredith MP, Chesnut CH III (2005) Vertebral fracture risk reduction with risedronate in post-menopausal women with osteoporosis: a meta-analysis of individual patient data. Aging Clin Exp Res 17:150–156
Harrington JT, Ste-Marie LG, Brandi ML, Civitelli R, Fardellone P, Grauer A, Barton I, Boonen S (2004) Risedronate rapidly reduces the risk for nonvertebral fractures in women with postmenopausal osteoporosis. Calcif Tissue Int 74:129–135
Stewart LA Tierney JF (2002) To IPD or not to IPD? Advantages and disadvantages of systematic reviews using individual patient data. Eval Health Prof 25:76–97
Smith CT, Williamson PR, Marson AG (2005) An overview of methods and empirical comparison of aggregate data and individual patient data results for investigating heterogeneity in meta-analysis of time-to-event outcomes. J Eval Clin Pract 11:468–478
Lambert PC, Sutton AJ, Abrams KR, Jones DR (2002) A comparison of summary patient-level covariates in meta-regression with individual patient data meta-analysis. J Clin Epidemiol 55:86–94
Chalmers I (1993) The Cochrane collaboration: preparing, maintaining, and disseminating systematic reviews of the effects of health care. Ann N Y Acad Sci 703:156–163
Grima DT, Burge RT, Becker DL, Tosteson AN (2002) Short-term cost-effectiveness of bisphosphonate therapies for postmenopausal osteoporotic women at high risk of fracture. P&T 27:448–455
Tosteson AN, Jonsson B, Grima DT, O'Brien BJ, Black DM, Adachi JD (2001) Challenges for model-based economic evaluations of postmenopausal osteoporosis interventions. Osteoporos Int 12:849–857
Papaioannou A, Wiktorowicz ME, Adachi JD, Goeree R, Papadimitropoulos E, Bedard M, Brazil K, Parkinson W, Weaver B (2000) Mortality, independence in living, and re-fracture, one year following hip fracture in Canadians. J Obstet Gynaecol Can 22:591–597
Kanis JA, Johnell O, De Laet C, Johansson H, Oden A, Delmas P, Eisman J, Fujiwara S, Garnero P, Kroger H, McCloskey EV, Mellstrom D, Melton LJ, Pols H, Reeve J, Silman A, Tenenhouse A (2004) A meta-analysis of previous fracture and subsequent fracture risk. Bone 35:375–382
Kanis JA, Johnell O, Oden A, Dawson A, De Laet C, Jonsson B (2001) Ten year probabilities of osteoporotic fractures according to BMD and diagnostic thresholds. Osteoporos Int 12:989–995
Papadimitropoulos EA, Coyte PC, Josse RG, Greenwood CE (1997) Current and projected rates of hip fracture in Canada. CMAJ 157:1357–1363
Melton LJ III, Lane AW, Cooper C, Eastell R, O'Fallon WM, Riggs BL (1993) Prevalence and incidence of vertebral deformities. Osteoporos Int 3:113–119
Melton LJ III, Crowson CS, O'Fallon WM (1999) Fracture incidence in Olmsted County, Minnesota: comparison of urban with rural rates and changes in urban rates over time. Osteoporos Int 9:29–37
Black DM, Palermo L, Grima DT (2006) Developing better economic models of osteoporosis: considerations for the calculation of the relative risk of fracture. Value Health 9:54–58
World Health Organization (2002) Estimates of child and adult mortality and life expectancy at birth by country. WHO, Geneva
Keene GS, Parker MJ, Pryor GA (1993) Mortality and morbidity after hip fractures. BMJ 307:1248–1250
Cranney A, Tugwell P, Wells G, Guyatt G (2002) Meta-analyses of therapies for postmenopausal osteoporosis. I. Systematic reviews of randomized trials in osteoporosis: introduction and methodology. Endocr Rev 23:496–507
Harris ST, Watts NB, Genant HK, McKeever CD, Hangartner T, Keller M, Chesnut CH III, Brown J, Eriksen EF, Hoseyni MS, Axelrod DW, Miller PD (1999) Effects of risedronate treatment on vertebral and nonvertebral fractures in women with postmenopausal osteoporosis: a randomized controlled trial. Vertebral Efficacy With Risedronate Therapy (VERT) Study Group. JAMA 282:1344–1352
Reginster J, Minne HW, Sorensen OH, Hooper M, Roux C, Brandi ML, Lund B, Ethgen D, Pack S, Roumagnac I, Eastell R (2000) Randomized trial of the effects of risedronate on vertebral fractures in women with established postmenopausal osteoporosis. Vertebral Efficacy with Risedronate Therapy (VERT) Study Group. Osteoporos Int 11:83–91
McClung MR, Bensen WG, Bolognese M et al (1998) Risedronate increases bone mineral density at the hip, spine and radius in postmenopausal women with low bone mass. Osteoporos Int 8:111
Fogelman I, Ribot C, Smith R, Ethgen D, Sod E, Reginster JY (2000) Risedronate reverses bone loss in postmenopausal women with low bone mass: results from a multinational, double-blind, placebo-controlled trial. BMD-MN Study Group. J Clin Endocrinol Metab 85:1895–1900
Hooper M, Ebeling P, Roberts A et al (1999) Risedronate prevents bone loss in early postmenopausal women. Calcif Tissue Int 64:S69
Cummings SR, Black DM, Thompson DE, Applegate WB, Barrett-Connor E, Musliner TA, Palermo L, Prineas R, Rubin SM, Scott JC, Vogt T, Wallace R, Yates AJ, LaCroix AZ (1998) Effect of alendronate on risk of fracture in women with low bone density but without vertebral fractures: results from the Fracture Intervention Trial. JAMA 280:2077–2082
Teramukai S, Matsuyama Y, Mizuno S, Sakamoto J (2004) Individual patient-level and study-level meta-analysis for investigating modifiers of treatment effect. Jpn J Clin Oncol 34:717–721
Shih W (2002) Problems in dealing with missing data and informative censoring in clinical trials. Curr Control Trials Cardiovasc Med 3:4
Altman DG, Bland JM (1998) Time to event (survival) data. BMJ 317:468–469
Williamson PR, Marson AG, Tudur C, Hutton JL, Chadwick D (2000) Individual patient data meta-analysis of randomized anti-epileptic drug monotherapy trials. J Eval Clin Pract 6:205–214
Delmas PD, Li Z, Cooper C (2004) Relationship between changes in bone mineral density and fracture risk reduction with antiresorptive drugs: some issues with meta-analyses. J Bone Miner Res 19:330–337
Wells G, Cranney A, Peterson J, Boucher M, Shea B, Robinson V, Coyle D, Tugwell P (2008) Risedronate for the primary and secondary prevention of osteoporotic fractures in postmenopausal women. Cochrane.Database.Syst.Rev. CD004523
Clemmesen B, Ravn P, Zegels B, Taquet AN, Christiansen C, Reginster JY (1997) A 2-year phase II study with 1-year of follow-up of risedronate (NE-58095) in postmenopausal osteoporosis. Osteoporos Int 7:488–495
Mortensen L, Charles P, Bekker PJ, Digennaro J, Johnston CC Jr. (1998) Risedronate increases bone mass in an early postmenopausal population: two years of treatment plus one year of follow-up. J Clin Endocrinol Metab 83:396–402
McClung MR, Geusens P, Miller PD, Zippel H, Bensen WG, Roux C, Adami S, Fogelman I, Diamond T, Eastell R, Meunier PJ, Reginster JY (2001) Effect of risedronate on the risk of hip fracture in elderly women. Hip Intervention Program Study Group. N Engl J Med 344:333–340
Disclaimers
This manuscript was funded by the Alliance for Better Bone Health, Procter & Gamble Pharmaceuticals Canada, and sanofi-aventis Canada Inc.
Conflicts of interest
Jonathan D. Adachi is a consultant for Amgen; Astra Zeneca, Eli Lilly; GlaxoSmithKline; Merck Frosst; Novartis; Proctor & Gamble; Roche; sanofi-aventis; Servier; and Wyeth (clinical trials: Eli Lilly; GlaxoSmithKline; Merck; Novartis; Pfizer; Proctor & Gamble; sanofi-aventis; Servier; and Wyeth). Alexandra Papaioannou is a consultant and adviser for Amgen, Eli Lilly, Merck Frosst, Novartis, Proctor & Gamble, sanofi-aventis, and Servier (clinical trials: Amgen, Eli Lilly, Merck, Novartis, Proctor & Gamble, and sanofi-aventis). William D. Leslie received speaker fees, research honoraria, and unrestricted research grants from Merck Frosst Canada Ltd; research honoraria and unrestricted educational grants from The Alliance for Better Bone Health: sanofi-aventis and Procter & Gamble Pharmaceuticals Canada, Inc.; unrestricted research grants from Novartis Pharmaceuticals Canada, Inc.; unrestricted educational grants from Genzyme Canada. Valery Walker is a paid consultant for Alliance for Better Bone Health, Procter & Gamble Pharmaceuticals Canada, and sanofi-aventis Canada Inc. Courtney C. Kennedy and George Ioannidis have no disclosures.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Adachi, J.D., Kennedy, C.C., Papaioannou, A. et al. Treating osteoporosis in Canada: what clinical efficacy data should be considered by policy decision makers?. Osteoporos Int 20, 1785–1793 (2009). https://doi.org/10.1007/s00198-009-0870-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-009-0870-9