
Abstract
Summary
This study assesses the possible association between poverty and osteoporosis and/or fragility fractures in a population of postmenopausal women. We found that postmenopausal women with low socioeconomic status had lower values of BMD at the lumbar spine, a higher prevalence of densitometric osteoporosis, and a higher prevalence of total and vertebral fractures.
Introduction
Some lifestyles are related to the presence of osteoporosis and/or fragility fractures, whereas poverty is related to some lifestyles. Because of this, we studied the possible association of poverty with osteoporosis and fractures.
Methods
This was an observational, cross-sectional study performed in the Canary Islands, Spain. Participants consisted of a total of 1,139 ambulatory postmenopausal women aged 50 years or older with no previous osteoporosis diagnosis and who were enrolled in some epidemiological studies. The prevalence of fractures (vertebral and non-vertebral) and the prevalence of osteoporosis (T-score <–2.5 either at the lumbar spine or the femoral neck). A previously validated questionnaire elicited the most important risk factors for osteoporosis: socioeconomic status, defined by the annual income was also assessed by a personal interview. A dorso-lateral X-ray of the spine was performed, and bone mineral density (BMD) was measured by DXA in the lumbar spine (L2–L4) and proximal femur.
Results
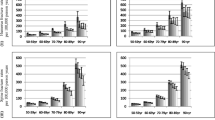
Compared to women with a medium and high socioeconomic status (n = 665), those who were classified into poverty (annual family income lower than 6,346.80 Euros, in a one-member family, n = 474), were older and heavier and had lower height, lower prevalence of tobacco and alcohol consumption, lower use of HRT and higher use of thiazides.
After correcting for age and body mass index (BMI), women in poverty had lower spine BMD values than women with a medium and high socioeconomic status (0.840 g/cm2 vs. 0.867 g/cm2, p = 0.005), but there were no statistical differences in femoral neck BMD between groups. The prevalence of osteoporosis was also higher in women in poverty [40.6% vs. 35.6%, (OR 1.35, CI 95%: 1.03; 1.76)] after adjusting by age and BMI. Moreover, 37.8% of women in poverty had a history of at least one fragility fracture compared to 27.7% of women not in poverty (OR: 1.45, CI 95%: 1.11; 1.90). The prevalence of vertebral fractures was also higher in women in poverty 24.7% vs. 13.4%, (OR 2.01, CI 95%: 1.44; 2.81).
Conclusions
Postmenopausal women with low socioeconomic status had lower values of BMD at the lumbar spine, and a higher prevalence of densitometric osteoporosis, and a higher prevalence of total and vertebral fractures. Because of this, apart from the well known risk factors for osteoporosis, poverty should be taken into account as a possible risk factor for both osteoporosis and fragility fractures, in order to establish sanitary strategies to protect unfavoured postmenopausal women.
Similar content being viewed by others


References
Melton LJ 3rd, Chrischilles EA, Cooper C, Lane AW, Riggs BL (1992) Perspective. How many women have osteoporosis? J Bone Miner Res 7:1005–1010
Pachucki-Hyde L (2001) Assessment of risk factors for osteoporosis and fracture. Nurs Clinics N Am 36:401–408 vii
Green AD, Colon-Emeric CS, Bastian L, Drake MT, Lyles KW (2004) Does this woman have osteoporosis? JAMA 292:2890–2900
Gourlay ML, Miller WC, Richy F, Garrett JM, Hanson LC, Reginster JY (2005) Performance of osteoporosis risk assessment tools in postmenopausal women aged 45–64 years. Osteoporos Int 16:921–927
Khan S, Murray RP, Barnes GE (2002) A structural equation model of the effect of poverty and unemployment on alcohol abuse. Addictive Behav 27:405–423
Wagenknecht LE, Perkins LL, Cutter GR, Sidney S, Burke GL, Manolio TA, Jacobs DR Jr, Liu KA, Friedman GD, Hughes GH et al (1990) Cigarette smoking behavior is strongly related to educational status: the CARDIA study. Prev Med 19:158–169
Lantz PM, House JS, Lepkowski JM, Williams DR, Mero RP, Chen J (1998) Socioeconomic factors, health behaviors, and mortality: results from a nationally representative prospective study of US adults. JAMA 279:1703–1708
Meara E (2006) Welfare reform, employment, and drug and alcohol use among low-income women. Harvard Rev Psychiatry 14:223–232
Winkleby MA, Fortmann SP, Barrett DC (1990) Social class disparities in risk factors for disease: eight-year prevalence patterns by level of education. Prev Med 19:1–12
Olson CM, Bove CF, Miller EO (2007) Growing up poor: long-term implications for eating patterns and body weight. Appetite 49:198–207
Osler M (1993) Social class and health behaviour in Danish adults: a longitudinal study. Public Health 107:251–260
Davey Smith G, Egger M (1993) Socioeconomic differentials in wealth and health. BMJ (Clinical research) 307:1085–1086
Haan M, Kaplan GA, Camacho T (1987) Poverty and health. Prospective evidence from the Alameda County Study. Am J Epidemiol 125:989–998
Miech RA, Kumanyika SK, Stettler N, Link BG, Phelan JC, Chang VW (2006) Trends in the association of poverty with overweight among US adolescents, 1971–2004. JAMA 295:2385–2393
Cooper C, O’Neill T, Silman A (1993) The epidemiology of vertebral fractures. European Vertebral Osteoporosis Study Group. Bone 14(Suppl 1):S89–S97
Sosa M, Hernandez D, Estevez S, Rodriguez M, Liminana JM, Saavedra P, Lainez P, Diaz P, Betancor P (1998) The range of bone mineral density in healthy Canarian women by dual X-ray absorptiometry radiography and quantitative computer tomography. J Clin Densitom 1:385–393
Sosa M, Saavedra P, Munoz-Torres M, Alegre J, Gomez C, Gonzalez-Macias J, Guanabens N, Hawkins F, Lozano C, Martinez M, Mosquera J, Perez-Cano R, Quesada M, Salas E (2002) Quantitative ultrasound calcaneus measurements: normative data and precision in the Spanish population. Osteoporos Int 13:487–492
World Health Organization Scientific Group (1981) Research on the Menopause, WHO Technical Services Report Series 670. Geneva: World Health Organization
Working Group on Protocols (2000) Basic data on osteoporosis. Rev Esp Enf Metab Óseas 9:84–85
Spanish National Institute of Statistics (2004) Life conditions questionnaire. Main results. INE. Avaiable at http://www.ine.es/prensa/np394pdf
Cummings SR, Block G, McHenry K, Baron RB (1987) Evaluation of two food frequency methods of measuring dietary calcium intake. Am J Epidemiol 126:796–802
Diaz Curiel M, Carrasco de la Pena JL, Honorato Perez J, Perez Cano R, Rapado A, Ruiz Martinez I (1997) Study of bone mineral density in lumbar spine and femoral neck in a Spanish population. Multicentre Research Project on Osteoporosis. Osteoporos Int 7:59–64
Genant HK, Wu CY, van Kuijk C, Nevitt MC (1993) Vertebral fracture assessment using a semiquantitative technique. J Bone Miner Res 8:1137–1148
Epstein S (2007) Is cortical bone hip? What determines cortical bone properties? Bone 41:S3–S8
Melton LJ 3rd, Eddy DM, Johnston CC Jr (1990) Screening for osteoporosis. Ann Intern Med 112:516–528
NIH Consensus Development Panel on Osteoporosis Prevention, Diagnosis and Therapy (2001). JAMA 285:785–795
Kay’s SK, Hindmarsh PC (2006) Catch-up growth: an overview. Pediatr Endocrinol Rev 3:365–378
Rivera JA, Sotres-Alvarez D, Habicht JP, Shamah T, Villalpando S (2004) Impact of the Mexican program for education, health, and nutrition (Progresa) on rates of growth and anemia in infants and young children: a randomized effectiveness study. JAMA 291:2563–2570
McLaren L (2007) Socioeconomic status and obesity. Epidemiologic Rev 29:29–48
Navarro MC, Saavedra P, Limiñana JM, Calvo JR, Betancor P, Sosa M (1997) Dietary calcium intake, bone mass and life-styles in postmenopausal women with and without osteoporosis. Rev Esp Nutr Comunit 3:15–24
Schroder H, Rohlfs I, Schmelz EM, Marrugat J (2004) Relationship of socioeconomic status with cardiovascular risk factors and lifestyle in a Mediterranean population. Eur J Nutr 43:77–85
Borrell C, Dominguez-Berjon F, Pasarin MI, Ferrando J, Rohlfs I, Nebot M (2000) Social inequalities in health related behaviours in Barcelona. J Epidemiol Commun Health 54:24–30
Wamala SP, Lynch J, Kaplan GA (2001) Women’s exposure to early and later life socioeconomic disadvantage and coronary heart disease risk: the Stockholm Female Coronary Risk Study. Int J Epidemiol 30:275–284
Giskes K, Kunst AE, Benach J, Borrell C, Costa G, Dahl E, Dalstra JA, Federico B, Helmert U, Judge K, Lahelma E, Moussa K, Ostergren PO, Platt S, Prattala R, Rasmussen NK, Mackenbach JP (2005) Trends in smoking behaviour between 1985 and 2000 in nine European countries by education. J Epidemiol Commun Health 59:395–401
Rossouw JE, Anderson GL, Prentice RL, LaCroix AZ, Kooperberg C, Stefanick ML, Jackson RD, Beresford SA, Howard BV, Johnson KC, Kotchen JM, Ockene J (2002) Risks and benefits of estrogen plus progestin in healthy postmenopausal women: principal results From the Women’s Health Initiative randomized controlled trial. JAMA 288:321–333
Wassertheil-Smoller S, Hendrix SL, Limacher M, Heiss G, Kooperberg C, Baird A, Kotchen T, Curb JD, Black H, Rossouw JE, Aragaki A, Safford M, Stein E, Laowattana S, Mysiw WJ (2003) Effect of estrogen plus progestin on stroke in postmenopausal women: the Women’s Health Initiative: a randomized trial. JAMA 289:2673–2684
Cummings SR, Melton LJ (2002) Epidemiology and outcomes of osteoporotic fractures. Lancet 359:1761–1767
Yang K, McElmurry BJ, Park CG (2006) Decreased bone mineral density and fractures in low-income Korean women. Health Care Women Int 27:254–267
Shatrugna V, Kulkarni B, Kumar PA, Rani KU, Balakrishna N (2005) Bone status of Indian women from a low-income group and its relationship to the nutritional status. Osteoporos Int 16:1827–1835
Pearson D, Taylor R, Masud T (2004) The relationship between social deprivation, osteoporosis, and falls. Osteoporos Int 15:132–138
Orces CH, Casas C, Lee S, Garci-Cavazos R, White W (2003) Determinants of osteoporosis prevention in low-income Mexican-American women. Southern Med J 96:458–464
Oslo Ministerial Declaration (2007) Global health: a pressing foreign policy issue of our time. Lancet 369:1373–1378
Acknowledgments
We would like to thank Professor L.J. Melton III of the Mayo Clinic, Rochester, Minesota, USA, for his constructive comments.
Conflicts of interest
None.
Author information
Authors and Affiliations
Corresponding author
Additional information
This study was support by an unrestricted grant of the Canarian Society of Osteoporosis (SOCAOS SL).
Rights and permissions
About this article
Cite this article
Navarro, M.C., Sosa, M., Saavedra, P. et al. Poverty is a risk factor for osteoporotic fractures. Osteoporos Int 20, 393–398 (2009). https://doi.org/10.1007/s00198-008-0697-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-008-0697-9