
Abstract
Summary
This study used in-depth interviews and focus groups to evaluate osteoporosis care after a fracture. Patients (eligible women aged 67 who sustained a clinical fracture(s)), clinicians, and staff stated that an outreach program facilitated osteoporosis care management, but more-tailored education and support and increased participation of orthopedic specialists appear necessary.
Introduction
Osteoporosis treatment reduces fracture risk, but screening and treatment are underutilized, even after a fracture has occurred. This study evaluated key stakeholder perspectives about the care of osteoporosis after a fracture.
Methods
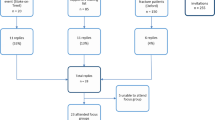
Participants were from a nonprofit health maintenance organization in the United States: eligible women members aged 67 or older who sustained a clinical fracture(s) (n = 10), quality and other health care managers (n = 20), primary care providers (n = 9), and orthopedic clinicians and staff (n = 28); total n = 67. In-depth interviews and focus groups elicited participant perspectives on an outreach program to patients and clinicians and other facilitators and barriers to care. Interviews and focus group sessions were transcribed and content-analyzed.
Results
Patients, clinicians, and staff stated that outreach facilitated osteoporosis care management, but important patient barriers remained. Patient knowledge gaps and fatalism were common. Providers stated that management needed to begin earlier, and longer-term patient support was necessary to address adherence. Orthopedic clinicians and staff expressed lack of confidence in their osteoporosis management but willingness to encourage treatment.
Conclusions
Although an outreach program assisted with the management of osteoporosis after a fracture, more-tailored education and support and increased participation of orthopedic specialists appear necessary to maximize osteoporosis management.
Similar content being viewed by others


References
National Osteoporosis Foundation (2000) Physicians guide to prevention and treatment of osteoporosis
Cummings SR, Melton LJ (2002) Epidemiology and outcomes of osteoporotic fractures. Lancet 359:1761–1767
Elliot-Gibson V, Bogoch ER, Jamal SA, Beaton DE (2004) Practice patterns in the diagnosis and treatment of osteoporosis after a fragility fracture: a systematic review. Osteoporos Int 15:767–778
Feldstein AC, Elmer PJ, Smith DH, Herson M, Orwoll E, Chen C, Aickin M, Swain MC (2006) Electronic medical record reminder improves osteoporosis management after a fracture: A randomized, controlled trial. J Am Geriatr Soc 54:450–457
Gardner MJ, Brophy RH, Demetrakopoulos D, Koob J, Hong R, Rana A, Lin JT, Lane JM (2005) Interventions to improve osteoporosis treatment following hip fracture. A prospective, randomized trial. J Bone Joint Surg Am 87:3–7
Majumdar SR, Rowe BH, Folk D, Johnson JA, Holroyd BH, Morrish DW, Maksymowych WP, Steiner IP, Harley CH, Wirzba BJ, Hanley DA, Blitz S, Russell AS (2004) A controlled trial to increase detection and treatment of osteoporosis in older patients with a wrist fracture. Ann Intern Med 141:366–373
Bliuc D, Eisman JA, Center JR (2006) A randomized study of two different information-based interventions on the management of osteoporosis in minimal and moderate trauma fractures. Osteoporos Int 17:1309–1317
Feldstein AC, Vollmer WM, Smith DH, Petrik A, Schneider J, Glauber H, Herson M (2007) An outreach program improved osteoporosis management after a fracture. J Am Geriatr Soc 55:1464–1469 [Epub 2007 Jul 30]
Ali NS, Twibell KR (1994) Barriers to osteoporosis prevention in perimenopausal and elderly women. Geriatr Nurs 15:201–205
Burgener M, Arnold M, Katz JN, Polinski JM, Cabral D, Avorn J, Solomon DH (2005) Older adults’ knowledge and beliefs about osteoporosis: results of semistructured interviews used for the development of educational materials. J Rheumatol 32:673–677
Jaglal SB, Cameron C, Hawker GA, Carroll J, Jaakkimainen L, Cadarette SM, Bogoch ER, Kreder H, Davis D (2006) Development of an integrated-care delivery model for post-fracture care in Ontario, Canada. Osteoporos Int 17:1337–1345
Freeborn DK, Pope C (1994) Promise and performance in managed care: the prepaid group practice model
Feldstein AC, Glasgow RE (2008) A practical, robust implementation and sustainability model (PRISM) for integrating research findings into practice. Joint Commission Journal on Quality and Patient Safety, March, In Press
Feldstein AC, Elmer PJ, Orwoll E, Herson M, Hillier T (2003) Bone mineral density measurement and treatment for osteoporosis in older individuals with fractures: A gap in evidence-based practice guideline. Arch Intern Med 163:2165–2172
Erlandson DA, Harris EL, Skipper BL, Allen SD (1993) Doing naturalistic inquiry: a guide to methods
Marshall C, Rossman GB (1995) Designing Qualitative Research. 2nd Edn
Lincoln YS, Guba EG (1985) Naturalistic Inquiry
Lofland l, Lofland J (1995) Analyzing Social Settings: A guide to qualitative observation and analysis. 3rd Edn
Wolcott HF (1994) Transforming Qualitative Data: Description, Analysis, and Interpretation
Strauss AL, Corbin JM (1990) Basics of qualitative research: Grounded theory procedures and techniques
Ettinger B, Pressman AR, Schein J, Chan J, Silver P, Connolly N (1998) Alendronate use among 812 women: Prevalence of gastrointestinal complaints, non-compliance with patient instructions, and discontinuation. J Manag Care Pharm 4:488–492
Jaglal SB, McIsaac WJ, Hawker G, Carroll J, Jaakkimainen L, Cadarette SM, Cameron C, Davis D (2003) Information needs in the management of osteoporosis in family practice: an illustration of the failure of the current guideline implementation process. Osteoporos Int 14:672–676
Jaglal SB, Carroll J, Hawker G, McIsaac WJ, Jaakkimainen L, Cadarette SM, Cameron C, Davis D (2003) How are family physicians managing osteoporosis? Qualitative study of their experiences and educational needs. Can Fam Physician 49:462–468 462–68
Blalock SJ, Currey SS, DeVellis RF, DeVellis BM, Giorgino KB, Anderson JJ, Dooley MA, Gold DT (2000) Effects of educational materials concerning osteoporosis on women’s knowledge, beliefs, and behavior. Am J Health Promot 14:161–169
Acknowledgments
We would like to acknowledge Martha Swain for editorial support and Debra Burch and Chalinya Bruce for secretarial support.
This study was supported in part by a research contract from Merck & Co., Inc.
This study was presented at the 13th Annual HMO Research Network Conference, March 19–21, 2007, Portland, Oregon, and the American Society of Bone and Mineral Research Meeting, September 16–19, 2007, Oahu, Hawaii.
Author information
Authors and Affiliations
Corresponding author
Additional information
Disclaimers: This study was supported in part by a research contract from Merck & Co., Inc. The sponsor had no role in the study design, methods, subject recruitment, data collection, analysis, or preparation of the paper.
Dr. Feldstein has received research grant support from Merck & Co, Inc.; Amgen; and Sanofi-Aventis. Dr. Vollmer has served on ad hoc advisory boards for Merck and Co., Inc., and is director of the Burden of Obstructive Lung Disease (BOLD) Operations Center, funding for which includes unrestricted educational grants to his employer, the Center for Health Research, Kaiser Permanente Northwest, from Boehringer Ingelheim, Pfizer, ALTANA, GlaxoSmithKline, AstraZeneca, Novartis, Chiesi, and Merck. Dr. Smith has received research grant support from Sanofi-Aventis, Abbot, Amgen, and Genzyme.
Appendix
Appendix
Rights and permissions
About this article
Cite this article
Feldstein, A.C., Schneider, J., Smith, D.H. et al. Harnessing stakeholder perspectives to improve the care of osteoporosis after a fracture. Osteoporos Int 19, 1527–1540 (2008). https://doi.org/10.1007/s00198-008-0605-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-008-0605-3