
Abstract
Summary
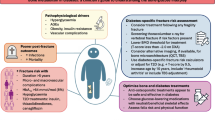
Risk of fragility fractures in older women appears to be under-recognized and under treated. Analysis of a national sample of older US women reveals that over 5 million are at high risk of fracture; only one third of these report being told they have osteoporosis and one quarter are receiving appropriate treatment.
Introduction
Substantial numbers of older women in the United States suffer fragility fractures each year. Although risk for these fractures can be readily identified from clinical characteristics, many women may not be receiving treatments demonstrated to reduce risk. Our objective was to estimate the extent of fracture risk among older white US women and assess patterns of use of pharmacologic agents in response to that risk.
Methods
Cross-sectional data from the National Health and Nutrition Examination Survey (NHANES) for 1999–2000 and 2001–2002 were combined to enumerate risk factors for fracture and use of antiresorptive prescription medications for all white women 65 years of age and older. The FRACTURE Index (FI), developed from the Study of Osteoporotic Fractures (SOF), which combines subjects’ characteristics to estimate five-year fracture risk, was applied to these national data.
Results
Of more than 15 million US women in this age group almost 40% have one risk factor in addition to age that predisposes to fracture; 20% have two or more. More than 5 million women are in the highest category of FI risk; 26% of these will have a nonvertebral fracture and 10% will have a vertebral fracture in the next five years. Antiresorptive medications are being taken by less than 50% of women in most risk categories when all antiresorptives, including estrogen replacement, are included; only 17% of older women who have sustained a prior fracture and 13% in the highest category of FI risk are receiving agents specifically intended to reduce bone loss.
Conclusions
Millions of older US women are at high risk for fragility fractures. Levels of treatment with antiresorptive medications are low and are not commensurate with fracture risk.
Similar content being viewed by others


References
National Osteoporosis Foundation (1998) Physician’s guide to prevention and treatment of osteoporosis. National Osteoporosis Foundation, Washington, DC
Brown JP, Josse RG (2002) 2002 clinical practice guidelines for the diagnosis and management of osteoporosis in Canada. CMAJ 167(10 Suppl):S1–S34, 12
Royal College of Physicians of London (1999) Osteoporosis clinical guidelines for prevention and treatment. Royal College of Physicians of London, London
Kanis JA, Delmas P, Burckhardt P, Cooper C, Torgerson D (1997) Guidelines for diagnosis and management of osteoporosis. The European foundation for osteoporosis and bone disease. Osteoporos Int 7:390–406
Black DM, Steinbuch M, Palermo L et al (2001) An assessment tool for predicting fracture risk in postmenopausal women. Osteoporos Int 12:519–528
Burger H, de Laet CE, Weel AE, Hofman A, Pols HA (1999) Added value of bone mineral density in hip fracture risk scores. Bone 25:369–374
McGrother CW, Donaldson MM, Clayton D, Abrams KR, Clarke M (2002) Evaluation of a hip fracture risk score for assessing elderly women: the Melton Osteoporotic Fracture (MOF) study. Osteoporos Int 13:89–96
Colon-Emeric CS, Pieper CF, Artz MB (2002) Can historical and functional risk factors be used to predict fractures in community-dwelling older adults? Development and validation of a clinical tool. Osteoporos Int 13:955–961
van Staa TP, Leufkens HG, Cooper C (2002) Utility of medical and drug history in fracture risk prediction among men and women. Bone 31:508–514
Elliot-Gibson V, Bogoch ER, Jamal SA, Beaton DE (2004) Practice patterns in the diagnosis and treatment of osteoporosis after a fragility fracture: a systematic review. Osteoporos Int 15:767–778
Centers for Disease Control and Prevention (CDC). National Center for Health Statistics (NCHS). National Health and Nutrition Examination Survey. Hyattsville, MD: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, [1999–2000, 2001–2002]
World Health Organization (1994) Assessment of fracture risk and its application to screening for osteoporosis. Technical Report Series 843. WHO, Geneva
Stone KL, Seeley DG, Lui LY et al (2003) BMD at multiple sites and risk of fracture of multiple types: long-term results from the study of osteoporotic fractures. J Bone Miner Res 18:1947–1954
Cummings SR, Black DM, Thompson DE et al (1998) Effect of alendronate on risk of fracture in women with low bone density but without vertebral fractures: results from the Fracture Intervention trial. JAMA 280:2077–2082, Dec 23–30
McClung MR, Geusens P, Miller PD et al (2001) Effect of risedronate on the risk of hip fracture in elderly women. Hip Intervention Program Study Group. N Engl J Med 344:333–340
Kanis JA, Johnell O, Black DM et al (2003) Effect of raloxifene on the risk of new vertebral fracture in postmenopausal women with osteopenia or osteoporosis: a reanalysis of the Multiple Outcomes of Raloxifene Evaluation trial. Bone 33:293–300
Lindsay R, Magowan S, Barton I, Felsenberg D, Adachi JD (2005) Risedronate demonstrates antifracture efficacy over a range of baseline BMD levels. Abstract (M367) ASBMR annual meeting Sept. 2005
Rossouw JE, Anderson GL, Prentice RL et al (2002) Risks and benefits of estrogen plus progestin in healthy postmenopausal women: principal results from the Women’s Health Initiative randomized controlled trial. JAMA 288:321–333
Acknowledgement
Supported by an unrestricted grant from the Alliance for Better Bone Health (Procter & Gamble Pharmaceuticals and sanofi-aventis).
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Gehlbach, S.H., Avrunin, J.S., Puleo, E. et al. Fracture risk and antiresorptive medication use in older women in the USA. Osteoporos Int 18, 805–810 (2007). https://doi.org/10.1007/s00198-006-0310-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-006-0310-z