
Abstract
Introduction
We determined the prevalence of left-right differences in hip bone mineral density (BMD) by dual-energy x-ray absorptiometry (DXA) and the resultant consequence, namely: the frequency at which patients would be classified differently if lumbar spine and only one hip (rather than both hips) were measured.
Methods
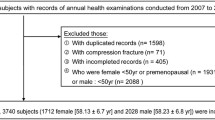
This was a retrospective DXA scan reanalysis of 3012 white women ≥50 yrs who had scans of both hips using Hologic DXA systems. The difference between left and right hips was considered significant if it exceeded the least significant change (LSC) for any of three hip subregions (total hip, femoral neck, trochanter). The number of women with osteoporosis in both hips, the left hip only, or the right hip only was determined by lowest T-score from total hip, femoral neck, or trochanter.
Results
Despite high left-right correlations of subregion BMD, significant left-right differences in BMD were common: the difference exceeded the LSC for 47% of women at total hip, 31% at femoral neck, and 56% at trochanter. Left-right differences in BMD that exceeded the LSC affected the percent agreement of left-right hip classification: for all women irrespective of spine status, there was 77% classification (diagnostic) agreement in hip pairs in which the left-right hip BMD difference exceeded the LSC versus 87% agreement in which LSC was not exceeded (significant difference in proportions, P<0.0001). The greatest risk of different classification would occur in women with normal spines as the diagnosis might be determined by hip T-scores. Using L1-4 lumbar spine T-scores, 1229 women were normal at the spine. Twenty-four (2%) were osteoporotic at both hips. However, 12 women (1%) were osteoporotic only in the left hip (significantly different from zero, P<0.001) and 11 (1%) only in the right hip (P<0.001); of these 23 women, the difference in BMD between the osteoporotic hip and the contralateral hip exceeded the LSC in 16 (70% of those with osteoporosis in only one hip). Using L1-4 lumbar spine T-scores, 1159 women were osteopenic at the spine. Of these, 126 (11%) were osteoporotic at both hips, 54 (5%) only in the left hip (P<0.001), and 42 (4%) only in the right hip (P<0.001); of these 96 women, the difference in BMD between the osteoporotic hip and the contralateral hip exceeded the LSC in 56 (58% of those with osteoporosis in only one hip).
Conclusions
A statistically significant number of women with osteoporosis are potentially classified differently when scanning only one hip as a result of the high prevalence of left-right differences in BMD. Although the percentages are low, the total number of women affected may be large. From a public health perspective, the practice of scanning both hips could potentially identify more women with osteoporosis and may help prevent future hip fractures.





Similar content being viewed by others

References
Blake GM, Wahner HW, Fogelman I (eds) (1999) The evaluation of osteoporosis: dual energy X-ray absorptiometry and ultrasound in clinical practice. Martin Dunitz, London, pp 53
Lessig HJ, Metzer MS, Siegel JA (1987) The symmetry of hip bone mineral density: a dual photon absorptiometry approach. Clin Nucl Med 12:811–812
Lilley J, Walters BG, Heath DA, Drolc Z (1992) Comparison and investigation of bone mineral density in opposing femora by dual energy x-ray absorptiometry. Osteoporos Int 2:274–278
Faulkner KG, Genant HK, McClung M (1995) Bilateral comparison of femoral bone density and hip axis length from single and fan beam DXA scans. Calcif Tissue Int 56:26–31
Bonnick SL, Nichols DL, Sanborn CF et al (1996) Right and left proximal femur analyses: Is there a need to do both? Calcif Tissue Int 58:307–310
Franck H, Munz M, Scherrer M (1997) Bone mineral density of opposing hips using dual energy x-ray absorptiometry in single beam and fan-beam design. Calcif Tissue Int 61:445–447
Yang RS, Tsai KS, Chieng PU, Liu Tk (1997) Symmetry of bone mineral density at the proximal femur with emphasis on the effect of side dominance. Calcif Tissue Int 61:189–191
Huddleston Al, Rockwell D, Kuland D (1980) Bone mass in lifetime tennis athletes. JAMA 244:1107–1109
Mazess RB, Nord RH, Hanson JA, Barden HS (2000) Bilateral measurement of femoral bone mineral density. J Clin Densitom 3(2):133–140
Rao AD, Reddy S, Rao DS (2000) Is there a difference between right and left femoral bone density? J Clin Densitom 3(1):57–61
Wong JCH, McEwan L, Lee N, Griffiths, Pocock NA (2003) The diagnostic role of dual femur bone density measurement in low impact fractures. Osteoporos Int 14:339–344
Petley GW, Taylor PA, Murrills AJ, Dennison E, Pearson G, Cooper C (2000) An investigation of the diagnostic values of bilateral femoral neck bone mineral density measurements. Osteoporos Int 11:675–679
Faulkner KG (2005) The tale of the T-score: review and perspective. Osteoporosis Int 16:347–352
Assessment of Fracture Risk and its Application to Screening for Postmenopausal Osteoporosis (1994) WHO Technical Report Series 843
Hamdy RC, Petak SA, Lenchik L (2002) Which dual x-ray absorptiometry skeletal sites and regions of interest should be used to determine the diagnosis of osteoporosis? J Clin Densitom 5(suppl 1):S11–S17
Lenchik L, Kiebzak GM, Blunt BA (2002) What is the role of serial bone mineral density measurements in patient management? J Clin Densitom 5(suppl 1):S29–S38
Hans D, Downs RW, Duboeuf F, Greenspan S, Jankowski LG, Kiebzak GM, Petak SM (2006) Skeletal sites for osteoporosis diagnosis: The 2005 ISCD Official Positions. J Clin Densitom 9(1):15–21
Zar JH (1984) Biostatistical analysis, 2nd edn. Prentice Hall, Englewood Cliffs, NJ, USA
Prince RL, Price RI, Ho S (1988) Forearm bone loss in hemiplegia: a model for the study of immobilization osteoporosis. J Bone Miner Res 3:305–310
Hamdy RC, Krishnaswamy G, Cancellarop V, Whalen Km, Harvill L (1993) Changes in bone mineral content and density after stroke. Am J Phys Med Rehab 4:188–191
Kiebzak GM, Lewiecki EM, Petak SM (2004) Good diagnostic agreement using T-scores between Delphi and Prodigy. J Clin Densitom 7(2):228
American Academy of Orthopaedic Surgeons website, http://www.AAOS.com
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Hamdy, R., Kiebzak, G.M., Seier, E. et al. The prevalence of significant left-right differences in hip bone mineral density. Osteoporos Int 17, 1772–1780 (2006). https://doi.org/10.1007/s00198-006-0192-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-006-0192-0