
Abstract
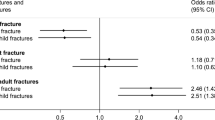
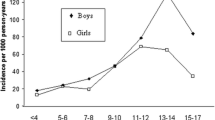
The aim of the study was to identify associations between fractures in childhood and family, anthropometric and lifestyle factors. Among 1,246 subjects aged 16.3–20.6 years (539 boys, 707 girls), based on a questionnaire, 869 were fracture-free while 377 (30.26%) had fractures. Of those reporting fractures, 146 reported multiple fractures (12% of studied population, 39% of all fractures). More boys had fractures than girls (35.6% vs 24.9%, p < 0.001). Fracture sites included: forearm (37%), fingers (23%) wrist (16%), ankle (14%), humerus (10%), tibia (8%) clavicle (7%) and femoral shaft / neck (3%). Among adolescents with multiple fractures, 52% also reported fractures in at least one family member, compared with 29% of those without a fracture history. Fractures in siblings and mothers (but not fathers) accounted for 44% of the liability in adolescents’ fractures. Subjects with multiple fractures reported more time at the computer than those without fractures and reported more time participating in team sports, and 18.6% avoided milk, whereas 12.4% of those without fractures reported milk-free diets. Using a logistic regression model, none of the lifestyle factors, except for computer use, were independently associated with fractures. Fractures, particularly multiple fractures, are common in childhood and adolescence. Familial clustering of fractures suggests shared genetic and environmental factors are responsible.

Similar content being viewed by others
References
Cummings SR, Melton LJ (2002) Epidemiology and outcomes of osteoporotic fractures. Lancet 359:1761–1767
Landin LA (1983) Fracture patterns in children. Analysis of 8,682 fractures with special reference to incidence, etiology and secular changes in a Swedish urban population 1950–1979. Acta Orthop Scand [Suppl] 202:1–109
Bailey DA, Wedge JH, McCulloch RG, Martin AD, Bernhardson SC (1989) Epidemiology of fractures of the distal end of the radius in children as associated with growth. J Bone Joint Surg Am 71:1225–1231
Jones IE, Cannan R, Goulding A (2000) Distal forearm fractures in New Zealand children: annual rates in a geographically defined area. N Z Med J 113:443–445
Jones G, Cooley HM (2002) Symptomatic fracture incidence in those under 50 years of age in southern Tasmania. J Paediatr Child Health 38:278–283
Landin LA (1997) Epidemiology of children’s fractures. J Pediatr Orthop B 6:79–83
Khosla S, Melton LJ 3rd, Dekutoski MB, Achenbach SJ, Oberg AL, Riggs BL (1997) Incidence of childhood distal forearm fractures over 30 years: a population-based study. JAMA 290:1479–1485
Lyons RA, Delahunty AM, Kraus D, Heaven M, McCabe M, Allen H, Nash P (1999) Children’s fractures: a population-based study. Inj Prev 5:129–132
Hagino H, Yamamoto K, Ohshiro H, Nose T (2000) Increasing incidence of distal radius fractures in Japanese children and adolescents. J Orthop Sci 5:356–360
Goulding A, Cannan R, Williams SM, Gold EJ, Taylor RW, Lewis-Barned NJ (1998) Bone mineral density in girls with forearm fractures. J Bone Miner Res 13:143–148
Jones IE, Williams SM, Goulding A (2004) Associations of birth weight and length, childhood size, and smoking with bone fractures during growth: evidence from a birth cohort study. Am J Epidemiol 159:343–350
Palczewska I, Niedzwiedzka Z (2001) Somatic development indices in children and youth of Warsaw. Med Wieku Rozwoj 5 [Suppl 1]:18–118
Ismail AA, O’Neill TW, Cockerill W, Finn JD, Cannata JB, Hoszowski K, Johnell O, Matthis C, Raspe H, Raspe A, Reeve J, Silman AJ (2000) Validity of self-report of fractures: results from a prospective study in men and women across Europe. EPOS Study Group. European Prospective Osteoporosis Study Group. Osteoporos Int 11:248–254
Riley AW (2004) Evidence that school-age children can self-report on their health. Ambul Pediatr 4 [Suppl]:371–376
Wills TA, Cleary SD (1997) The validity of self-reports of smoking: analyses by race/ethnicity in a school sample of urban adolescents. Am J Public Health 87:56–61
Craig CL, Marshall AL, Sjostrom M, Bauman AE, Booth ML, Ainsworth BE, Pratt M, Ekelund U, Yngve A, Sallis JF, Oja P (2003) International physical activity questionnaire: 12-country reliability and validity. Med Sci Sports Exerc 35:1381–1395
Jones IE, Williams SM, Dow N, Goulding A (2002) How many children remain fracture-free during growth? A longitudinal study of children and adolescents participating in the Dunedin Multidisciplinary Health and Development study. Osteoporos Int 13:990–995
Cheng JC, Shen WY (1993) Limb fracture pattern in different pediatric age groups: a study of 3,350 children. J Orthop Trauma 7:15–22
Hedlund R, Lindgren U (1986) The incidence of femoral shaft fractures in children and adolescents. J Pediatr Orthop 6:47–50
Brudvik C, Hove LM (2003) Childhood fractures in Bergen, Norway: identifying high-risk groups and activities. J Pediatr Orthop 23:629–634
Powell EC, Tanz RR (1996) In-line skate and roller-skate injuries in childhood. Pediatr Emerg Care 12:259–262
Jones IE, Taylor RW, Williams SM, Manning PJ, Goulding A (2002) Four-year gain in bone mineral in girls with and without past forearm fractures: a DXA study. Dual energy X-ray absorptiometry. J Bone Miner Res 17:1065–1072
Davidson P, Goulding A, Chalmers D (2003) Biomechanical analysis of arm fracture in obese boys. J Paediatr Child Health 39:657–664
Goulding A, Jones IE, Taylor RW, Williams SM, Manning PJ (2001) Bone mineral density and body composition in boys with distal forearm fractures: a dual-energy X-ray absorptiometry study. J Pediatr 139:509–515
Mallmin H, Ljunghall S, Persson I, Naessen T, Krusemo UB, Bergstrom R (1993) Fracture of the distal forearm as a forecaster of subsequent hip fracture: a population-based cohort study with 24 years of follow-up. Calcif Tissue Int 52:269–272
van Staa TP, Leufkens HG, Cooper C (2002) Does a fracture at one site predict later fractures at other sites? A British cohort study. Osteoporos Int 13:624–629
Cuddihy MT, Gabriel SE, Crowson CS, O’Fallon WM, Melton LJ 3rd (1999) Forearm fractures as predictors of subsequent osteoporotic fractures. Osteoporos Int 9:469–475
Olsson C, Nordqvist A, Petersson CJ (2004) Increased fragility in patients with fracture of the proximal humerus: a case control study. Bone 34:1072–1077
Goulding A, Jones IE, Taylor RW, Manning PJ, Williams SM (2000) More broken bones: a 4-year double cohort study of young girls with and without distal forearm fractures. J Bone Miner Res 15:2011–2018
Cardon LR, Garner C, Bennett ST, Mackay IJ, Edwards RM, Cornish J, Hegde M, Murray MA, Reid IR, Cundy T (2000); Evidence for a major gene for bone mineral density in idiopathic osteoporotic families. J Bone Miner Res 15:1132–1137
Fox KM, Cummings SR, Powell-Threets K, Stone K (1998) Family history and risk of osteoporotic fracture. Study of Osteoporotic Fractures Research Group. Osteoporos Int 8:557–562
Ma DQ, Jones G (2002) Clinical risk factors but not bone density are associated with prevalent fractures in prepubertal children. J Paediatr Child Health 38:497–500
Matsumoto K, Miyamoto K, Sumi H, Sumi Y, Shimizu K (2002) Upper extremity injuries in snowboarding and skiing: a comparative study. Clin J Sport Med 12:354–359
Blimkie CJ, Lefevre J, Beunen GP, Renson R, Dequeker J, Van Damme P (1993) Fractures, physical activity, and growth velocity in adolescent Belgian boys. Med Sci Sports Exerc 25:801–808
Dovey SM, Reeder AI, Chalmers DJ (1998) Continuity and change in sporting and leisure time physical activities during adolescence. Br J Sports Med 32:53–57
Ma D, Jones G (2003) Television, computer, and video viewing; physical activity; and upper limb fracture risk in children: a population-based case control study. J Bone Miner Res 18:1970–1977
Goulding A, Rockell JE, Black RE, Grant AM, Jones IE, Williams SM (2004) Children who avoid drinking cow’s milk are at increased risk for prepubertal bone fractures. J Am Diet Assoc 104:250–253
Wyshak G, Frisch RE (1994) Carbonated beverages, dietary calcium, the dietary calcium/phosphorus ratio, and bone fractures in girls and boys. J Adolesc Health 15:210–215
Van Staa TP, Bishop N, Leufkens HG, Cooper C (2004) Are inhaled corticosteroids associated with an increased risk of fracture in children? Osteoporos Int 15(10):785-791. E-pub 2004 Feb 21
Acknowledgments
We would like to thank Dr. Sandra Iuliano-Burns and Ms. Sheila Matthews from the Department of Medicine and Endocrinology, Austin Health, University of Melbourne, for their editing assistance in this article
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Konstantynowicz, J., Bialokoz-Kalinowska, I., Motkowski, R. et al. The characteristics of fractures in Polish adolescents aged 16–20 years. Osteoporos Int 16, 1397–1403 (2005). https://doi.org/10.1007/s00198-005-1850-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-005-1850-3