
Abstract
Introduction and hypothesis
The objective was to determine the relationship between the preoperative D-point and apical outcomes at 24 months, using the Operations and Pelvic Muscle Training in the Management of Apical Support Loss (OPTIMAL) dataset.
Methods
This was a secondary analysis of the OPTIMAL trial, a randomized multi-centered study comparing outcomes of sacrospinous ligament fixation and transvaginal uterosacral ligament suspension (USLS). The 2-year dataset utilized included women undergoing USLS with concomitant hysterectomy. The primary outcome was the relationship between preoperative D-point and apical outcomes at 24 months. Secondary objectives were to determine the relationship between preoperative D-point and anatomical, composite and subjective outcomes, and to determine a D-point cut-off that could be used to predict success in each of these categories.
Results
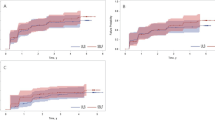
Of the 186 women in the USLS arm, 120 were available for analysis of anatomical failure at 24 months. A higher preoperative D-point correlated with improved apical outcome (C-point) at 24 months (r = 0.34; p value = 0.0002). Using ROC curves, a moderate association was found between the preoperative D-point and apical and anatomical success, (AUC 0.689 and 0.662). There was no relationship between preoperative D-point and composite or subjective success (AUC 0.577 and 0.458). Based on the ROC curves, a “cut-off” D-point value of −4.25 cm (sensitivity = 0.58, specificity = 0.67) was determined to be a predictor of postoperative anatomical success at 2 years.
Conclusions
Preoperative D-point correlates with postoperative anatomical and apical support, but is less successful at predicting subjective outcomes. The strongest predictive D-point cut-off for anatomical and apical success at 24 months was −4.25 cm.



Similar content being viewed by others


References
Margulies RU, Rogers M a M, Morgan DM. Outcomes of transvaginal uterosacral ligament suspension: systematic review and metaanalysis. Am J Obstet Gynecol. 2010;202:124–34. https://doi.org/10.1016/j.ajog.2009.07.052.
Richter LA, Park AJ, Boileau JE, et al. Does pelvic organ prolapse quantification examination D POint predict uterosacral ligament suspension outcomes? Female Pelvic Med Reconstr Surg. 2016;22:146–50.
Barber MD, Brubaker L, Burgio KL, et al. Comparison of 2 transvaginal surgical approaches and perioperative behavioral therapy for apical vaginal prolapse: the OPTIMAL randomized trial. JAMA. 2014;311:1023–34. https://doi.org/10.1001/jama.2014.1719.
Whiteside JL, Weber AM, L a M, Walters MD. Risk factors for prolapse recurrence after vaginal repair. Am J Obstet Gynecol. 2004;191:1533–8. https://doi.org/10.1016/j.ajog.2004.06.109.
Barber MD, Brubaker L, Burgio KL, et al. Comparison of 2 transvaginal surgical approaches and perioperative behavioral therapy for apical vaginal prolapse: the OPTIMAL randomized trial. JAMA. 2014;1023–34(16):311.
Barber MD, Brubaker L, Menefee S, et al. Operations and pelvic muscle training in the Management of Apical Support Loss (OPTIMAL) trial: design and methods. Contemp Clin Trials. 2009;30:178–89.
Shull BL, Bachofen C, Coates KW, Kuehl TJ. A transvaginal approach to repair of apical and other associated sites of pelvic organ prolapse with uterosacral ligaments. Am J Obstet Gynecol. 2000;183:1365–74.
Haylen BT, de Ridder D, Freeman RM, et al. An International Urogynecological Association (IUGA)/International Continence Society (ICS) Joint Report on the Terminology for Female Pelvic Floor Dysfunction. Int Urogynecol J. 2010;20:4–20. https://doi.org/10.1002/nau.
Bump RC, Mattiasson A, Kari B, et al. The standardization of terminology of female pelvic organ prolapse and pelvic floor dysfunction. Am J Obstet Gynecol. 1996;175(1):10–7.
Lowder JL, Oliphant SS, Shepherd JP, Ghetti C, Sutkin G. Genital hiatus size is associated with and predictive of apical vaginal support loss. Am J Obstet Gynecol. 2016;214:718.
Sutkin G, Zyczynski H, Sridhar A, Jelovsek K, Rardin C, Mazloomdoost D, et al. Posterior repair does not affect the success of transvaginal repair of apical prolapse. Am J Obstet Gynecol. 2019;220:S688–9.
Carter-Brooks CM, Lowder JL, Du AL, Lavelle ES, Giugale LE, Shepherd JP. Restoring genital hiatus to normative values after apical suspension alone versus with level 3 support procedures. Female Pelvic Med Reconstr Surg. 2019;25:226–30.
Vaughan MH, Siddiqui NY, Newcomb LK, et al. Surgical alteration of genital hiatus size and anatomic failure after vaginal vault suspension. Obstet Gynecol. 2018;131:1137–44.
Author information
Authors and Affiliations
Contributions
L.A. Richter: protocol/project development, data analysis, manuscript writing; S.E. Bradley: project development, data analysis, manuscript editing; A.J. Park: protocol/project development, manuscript editing; H.E. Richter: protocol/project development review, manuscript editing; S. Desale: data analysis; C.B. Iglesia: protocol/project development, manuscript editing.
Corresponding author
Ethics declarations
Conflicts of interest
Holly E. Richter: no conflicts of interest. Disclosures: Renovia—research funding (SUI, FI), Allergan—research funding (UUI), UpToDate—Royalties, NIA—research funding, NICHD—research funding, Obstet Gynecol and IUJ—travel reimbursement related to editor duties, Worldwide Fistula Fund—board; DSMB Bluewind, Symposia Medicus—CME speaker. Amy J. Park: speaker for Allergan, UpToDate royalties. Cheryl B. Iglesia: UpToDate contributor. None of the other authors has any conflicts of interest.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Richter, L.A., Bradley, S.E., Desale, S. et al. Association of Pelvic Organ Prolapse Quantification examination D point with uterosacral ligament suspension outcomes: the “OPTIMAL” D point. Int Urogynecol J 32, 2179–2184 (2021). https://doi.org/10.1007/s00192-021-04687-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00192-021-04687-0