
Abstract
Purpose
To investigate the clinical outcome and magnetic resonance imaging (MRI) findings after arthroscopic Bankart repair with additional double anchor footprint fixation (DAFF) at the 4 o’clock position, where the native footprint is widest anatomically, for recurrent anterior shoulder instability.
Methods
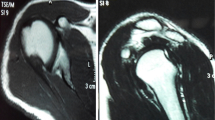
Forty-two patients (mean age 27.0 years) with recurrent anterior shoulder instability and without severe glenoid bone defects underwent arthroscopic Bankart repair with additional DAFF at the 4 o’clock position. Using three standard portals, single-row repair was performed at the 2, 3, and 5 o’clock positions, and DAFF with the suture bridging technique was conducted at the 4 o’clock position. MRI was performed preoperatively and at 6 months postoperatively. Patients with follow-up periods of ≥1 year were included in the present study and clinically evaluated at the final follow-up. The morphology at the 2 and 4 o’clock positions on radial MRI slices was compared between the preoperative and 6-month postoperative scans, and the footprint of the repaired capsulolabral complex at 6 months postoperatively was compared between the 2 and 4 o’clock positions.
Results
The average follow-up period was 19.5 ± 6.2 months. The rates of dislocation recurrence and positive apprehension test results were 2.4 and 4.8%, respectively. External rotation was restricted by 3.5°. The University of California at Los Angeles and Rowe scores at the final follow-up were 34.5 ± 1.0 points and 97.2 ± 5.7 points, respectively, representing significant improvements over the preoperative scores (p < 0.01). Although the capsulolabral complex at 6 months postoperatively was firmly repaired at both the 2 and 4 o’clock positions compared to its preoperative state, the footprint of the restored capsulolabral complex was wider at the 4 o’clock position than at the 2 o’clock position (p < 0.01).
Conclusions
Additional DAFF at the 4 o’clock position improved the glenohumeral stability and function of the shoulder joint. This study suggests that this technique is a reliable and useful treatment for shoulder instability.
Level of evidence
IV.



Similar content being viewed by others


References
Kim KC, Rhee KJ, Shin HD, Kim YM (2008) Arthroscopic separate labral repair and capsular plication with a suture anchor. Arch Orthop Trauma Surg 128:535–538
Magit DP, Tibone JE, Lee TQ (2008) In vivo comparison of changes in glenohumeral translation after arthroscopic capsulolabral reconstructions. Am J Sports Med 36:1389–1396
Moya D, Aydin N, Yamamoto N, Simone JP, Robles PP, Tytherleigh-Strong G et al (2021) Current concepts in anterior glenohumeral instability: diagnosis and treatment. SICOT J 7:48
DeFroda S, Bokshan S, Stern E, Sullivan K, Owens BD (2017) Arthroscopic Bankart Repair for the management of anterior shoulder instability: indications and outcomes. Curr Rev Musculoskelet Med 10:442–451
Hurley ET, Davey MS, Mojica ES, Fried JW, Gaafar M, Pauzenberger L et al (2021) Evaluation of factors associated with successful 5-year outcomes following arthroscopic Bankart repair in athletes. Knee Surg Sports Traumatol Arthrosc. https://doi.org/10.1007/s00167-021-06803-5
Memon M, Kay J, Cadet ER, Shahsavar S, Simunovic N, Ayeni OR (2018) Return to sport following arthroscopic Bankart repair: a systematic review. J Shoulder Elbow Surg 27:1342–1347
Miura K, Tsuda E, Tohyama H, Iwahori Y, Mae T, Mochizuki Y et al (2018) Can arthroscopic Bankart repairs using suture anchors restore equivalent stability to open repairs in the management of traumatic anterior shoulder dislocation? A meta-analysis. J Orthop Sci 23:935–941
Delgrande D, Lonjon G, Hardy P, Schoch B, Werthel JD (2021) Long-term results of arthroscopic Bankart repairs for anterior instability of the shoulder in patients aged thirty years or older. Int Orthop 45:1583–1589
Hasegawa Y, Kawasaki T, Nojiri S, Sobue S, Kaketa T, Gonda Y et al (2019) The number of injury events associated with the critical size of bipolar bone defects in rugby players with traumatic anterior shoulder instability. Am J Sports Med 47:2803–2808
Yamamoto N, Shinagawa K, Hatta T, Itoi E (2020) Peripheral-track and central-track hill-Sachs lesions: a new concept of assessing an on-track lesion. Am J Sports Med 48:33–38
Greenstein AS, Chen RE, Knapp E, Brown AM, Roberts A, Awad HA et al (2021) A biomechanical, cadaveric evaluation of single- versus double-row repair techniques on stability of Bony Bankart Lesions. Am J Sports Med 49:773–779
Iwaso H, Uchiyama E, Sakakibara S, Fukui N (2011) Modified double-row technique for arthroscopic Bankart repair: surgical technique and preliminary results. Acta Orthop Belg 77:252–257
Lafosse L, Baier GP, Jost B (2006) Footprint fixation for arthroscopic reconstruction in anterior shoulder instability: the Cassiopeia double-row technique. Arthroscopy 22:231e1-231e6
Moran CJ, Fabricant PD, Kang R, Cordasco FA (2014) Arthroscopic double-row anterior stabilization and bankart repair for the “high-risk” athlete. Arthrosc Tech 3:e65-71
Ahmad CS, Galano GJ, Vorys GC, Covey AS, Gardner TR, Levine WN (2009) Evaluation of glenoid capsulolabral complex insertional anatomy and restoration with single- and double-row capsulolabral repairs. J Shoulder Elbow Surg 18:948–954
Kim DS, Yoon YS, Chung HJ (2011) Single-row versus double-row capsulolabral repair: a comparative evaluation of contact pressure and surface area in the capsulolabral complex-glenoid bone interface. Am J Sports Med 39:1500–1506
Itoigawa Y, Itoi E, Sakoma Y, Yamamoto N, Sano H, Kaneko K (2012) Attachment of the anteroinferior glenohumeral ligament-labrum complex to the glenoid: an anatomic study. Arthroscopy 28:1628–1633
Itoigawa Y, Hooke AW, Sperling JW, Steinmann SP, Zhao KD, Itoi E et al (2019) The effect of subscapularis muscle contraction on coaptation of anteroinferior glenohumeral ligament-labrum complex after Bankart repair. J Biomech 85:134–140
Kawasaki T, Hasegawa Y, Kaketa T, Shiota Y, Gonda Y, Sobue S et al (2018) Midterm clinical results in rugby players treated with the Bristow procedure. Am J Sports Med 46:656–662
Liu T, Yamamoto N, Shinagawa K, Hatta T, Itoi E (2019) Curved-guide system is useful in achieving optimized trajectory for the most inferior suture anchor during arthroscopic Bankart repair. J Shoulder Elbow Surg 28:1692–1698
Sugaya H, Takahashi N (2016) Arthroscopic Osseous Bankart Repair in the Treatment of Recurrent Anterior Glenohumeral Instability. JBJS Essent Surg Tech 6:e26
Stein T, Mehling AP, Reck C, Buckup J, Efe T, Hoffmann R et al (2011) MRI assessment of the structural labrum integrity after Bankart repair using knotless bio-anchors. Knee Surg Sports Traumatol Arthrosc 19:1771–1779
Yoo JC, Lee YS, Tae SK, Park JH, Park JW, Ha HC (2008) Magnetic resonance imaging appearance of a repaired capsulolabral complex after arthroscopic bankart repair. Am J Sports Med 36:2310–2316
Ganokroj P, Keyurapan E (2019) Arthroscopic Bony Bankart repair using a double-row double-pulley technique. Arthrosc Tech 8:e31–e36
Wade R, Reddy PVB (2018) Functional outcome of arthroscopic double row repair for Bankart lesion. J Orthop 15:792–797
Buchmann S, Brucker PU, Beitzel K, Bock J, Eiber M, Wortler K et al (2016) Long-term effects on subscapularis integrity and function following arthroscopic shoulder stabilization with a low anteroinferior (5:30 o’clock) portal. Knee Surg Sports Traumatol Arthrosc 24:422–429
Jazini E, Shiu B, Robertson A, Russell JP, Iacangelo A, Henn RF 3rd et al (2016) A biomechanical analysis of anchor placement for Bankart Repair: effect of portal placement. Orthopedics 39:e323-327
McDonald LS, Thompson M, Altchek DW, McGarry MH, Lee TQ, Rocchi VJ et al (2016) Double-row capsulolabral repair increases load to failure and decreases excessive motion. Arthroscopy 32:2218–2225
Yousif MJ, Bicos J (2017) Biomechanical comparison of single- versus double-row capsulolabral repair for shoulder instability: a review. Orthop J Sports Med 5:2325967117742355
Hayashida K, Yoneda M, Mizuno N, Fukushima S, Nakagawa S (2006) Arthroscopic Bankart repair with knotless suture anchor for traumatic anterior shoulder instability: results of short-term follow-up. Arthroscopy 22:620–626
Shibata H, Gotoh M, Mitsui Y, Kai Y, Nakamura H, Kanazawa T et al (2014) Risk factors for shoulder re-dislocation after arthroscopic Bankart repair. J Orthop Surg Res 9:53
Acknowledgements
The authors would like to thank Enago (www.enago.jp) for the English language review. We thank Dr. Tomoki Wada and Dr. Yoshinori Gonda for their technical assistance.
Funding
This study was supported (in part) by a Grant‐in‐Aid for Young Scientists (No: 18K18371).
Author information
Authors and Affiliations
Contributions
YI: First author and corresponding author who contributed for all of this study; HU: Data acquisition; AK; Analysis of data; DM: Study design and data acquisition; TK: Analysis of data and data acquisition; YS: Data acquisition; YM: Conception of study and Interpretation of data; MI: Interpretation of data and Study design.
Corresponding author
Ethics declarations
Conflict of interest
We have no potential conflict of interest.
Ethical approval
The patients signed an informed consent form approved by the Institutional Review Board at Juntendo university (Juntendo University Urayasu Hospital, No. 30-017).
Informed consent
The patients provided written informed consent approved by the Institutional Review Board at Juntendo university.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Itoigawa, Y., Uehara, H., Koga, A. et al. Arthroscopic Bankart repair with additional footprint fixation using the double-row technique at the 4 o'clock position anatomically restored the capsulolabral complex and showed good clinical results. Knee Surg Sports Traumatol Arthrosc 30, 3827–3834 (2022). https://doi.org/10.1007/s00167-022-06974-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-022-06974-9