
Abstract
Purpose
Quadriceps tendon (QT) autograft ACL reconstruction was hypothesized to possess less anterior knee laxity, pivot shift laxity, and lower failure rates than hamstring tendon (HT) autografts.
Methods
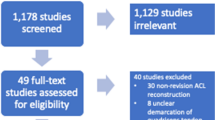
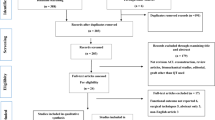
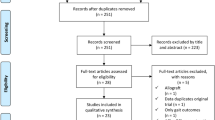
Terms “hamstring tendon autograft” and “ACL reconstruction” or “quadriceps tendon autograft” and “ACL reconstruction” were searched in Embase and PubMed. Inclusion criteria required that studies included patients treated for primary ACL injury with reconstruction using either a QT autograft (Group 1) or a HT autograft (Group 2) and instrumented anterior knee laxity assessment. Extracted information included surgical fixation method, graft type, graft thickness or diameter, single vs. double bundle surgical method, publication year, time between the index knee injury and surgery, % women, initial and final subject number, subject age, follow-up length, side-to-side anterior knee laxity difference, Lysholm Score, Subjective IKDC score, anterior knee laxity side-to-side difference grade, ipsilateral pivot shift laxity grade, and failure rate. The Methodological Index for Nonrandomized Studies was used to evaluate study methodological quality.
Results
The QT group (Group 1) had 17 studies and the HT group (Group 2) had 61 studies. Overall, Group 2 had greater pivot shift laxity (OR 1.29, 95% CI 1.05–1.59, p = 0.005). Group 2 suspensory femoral fixation had greater pivot shift laxity (OR 1.26, 95% CI 1.01–1.58, p = 0.02) than Group 1 compression femoral fixation. Group 2 compression femoral fixation also had more anterior knee laxity (OR 1.25, 95% CI 1.03–1.52, p = 0.01) than Group 1 compression femoral fixation and higher failure rates based on initial (OR 1.69, 95% CI 1.18–2.4, p = 0.002) and final (OR 1.89, 95% CI 1.32–2.71, p = 0.0003) subject number. Failure rate for HT compression femoral fixation was greater than suspensory femoral fixation based on initial (OR 2.08, 95% CI 1.52–2.84, p < 0.0001) and final (OR 2.26, 95% CI 1.63–3.16, p < 0.0001) subject number.
Conclusions
Overall, QT autografts had less pivot shift laxity and lower failure rates based on final subject number than HT autografts. Compression QT autograft femoral fixation had lower pivot shift laxity than suspensory HT autograft femoral fixation. Compression QT autograft femoral fixation had less anterior knee laxity and lower failure rates than compression HT autograft femoral fixation. Suspensory HT autograft femoral fixation had lower failure rates than compression HT autograft femoral fixation. Greater knee laxity and failure rates may be related to a combination of HT autograft diameter and configuration (tissue quality and dimensions, strands, bundles, and suturing method) variability and fixation mode.
Level of evidence
Level IV.



Similar content being viewed by others
References
Abraham NS, Byrne CJ, Young JM, Solomon MJ (2010) Meta-analysis of well-designed nonrandomized comparative studies of surgical procedures is as good as randomized controlled trials. J Clin Epidemiol 63:238–245
Akobeng AK (2005) Understanding systematic reviews and meta-analysis. Arch Dis Child 90:845–848
Ashford WB, Kelly TH, Chapin RW, Xerogeanes JW, Slone HS (2018) Predicted quadriceps vs. quadrupled hamstring tendon graft sizing using 3-dimensional MRI. Knee 25:1100–1106
Belk JW, Kraeutler MJ, Marshall HA, Goodrich JA, McCarty EC (2018) Quadriceps tendon autograft for primary anterior cruciate ligament reconstruction: a systematic review of comparative studies with minimum 2-year follow-up. Arthroscopy 34:1699–1707
Berman NG, Parker RA (2002) Meta-analysis: neither quick nor easy. BMC Med Res Methodol 2:10
Boniello MR, Schwingler PM, Bonner JM, Robinson SP, Cotter A, Bonner KF (2015) Impact of hamstring graft diameter on tendon strength: a biomechanical study. Arthroscopy 31:1084–1090
Collins NJ, Misra D, Felson DT, Crossley KM, Roos EM (2011) Measures of Knee Function International Knee Documentation Committee (IKDC) Subjective Knee Evaluation Form, Knee Injury and Osteoarthritis Outcome Score (KOOS), Knee Injury and Osteoarthritis Outcome Score Physical Function Short Form (KOOS-PS), Knee Outcome Survey Activities of Daily Living Scale (KOS-ADL), Lysholm Knee Scoring Scale, Oxford Knee Score (OKS), Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC), Activity Rating Scale (ARS), and Tegner Activity Score (TAS). Arthritis Care Res (Hoboken) 63(Suppl 11):S208–S228
Elmlinger BS, Nyland JA, Tillett ED (2006) Knee flexor function 2 years after anterior cruciate ligament reconstruction with semitendinosus-gracilis autografts. Arthroscopy 22:650–655
Galaviz KI, Weber MB, Straus A, Haw JS, Venkat Narayan KM, Kumail Ali M (2018) Global diabetes prevention interventions: a systematic review and network meta-analysis of real-world impact on incidence, weight and glucose. Diabetes Care 41:1526–1534
Harris JD, Brand JC, Cote MP, Dhawan A (2017) Research pearls: the significance of statistics and the perils of pooling. Part 3: pearls and pitfalls of meta-analyses and systematic reviews. Arthroscopy 33:1594–1602
Higgins JPT, Thompson SG, Deeks JJ, Altman DG (2003) Measuring inconsistency in meta-analyses. BMJ 327:557–560
Huedo-Medina TB, Sanchez-Meca J, Marin-Martinez F, Botella J (2006) Assessing heterogeneity in meta-analysis: Q statistic or I2 index? Psychol Methods 11:193–206
Ioannidis J, Patsopoulos N, Evangelou E (2007) Uncertainty in heterogeneity estimates in meta-analyses. BMJ 335:914–918
Israel H, Richter RR (2011) A guide to understanding meta-analysis. J Orthop Sports Phys Ther 41:496–504
Kanakamedala AC, Obioha OA, Arakgi ME, Schmidt PB, Lesniak BP, Musahl V (2019) No difference between full thickness and partial thickness quadriceps tendon autografts in anterior cruciate ligament reconstruction: a systematic review. Knee Surg Sports Traumatol Arthrosc 27:105–116
Kautzner J, Držík M, Handl M, Povýšil C, Kos P, Trč T, Havlas V (2017) Structural damage to the hamstring graft due to interaction with fixation material and its effect on biomechanical properties of ACL reconstruction. Acta Chir Orthop Traumatol Cech 84:101–105
Larson CM, Bedi A, Dierich ME, Swaringen JC, Wulf CA, Rowley DM, Giveans MR (2017) Generalized hypermobility, knee hyperextension, and outcomes after anterior cruciate ligament reconstruction: prospective, case-control study with mean 6 year follow-up. Arthroscopy 33:1852–1858
Levange PK (2001) Application and interpretation of simple odds ratios in physical therapy-related research. J Orthop Sports Phys Ther 31:496–503
Mae T, Shino K, Nakagawa S, Take Y, Hiramatsu K, Yoshikawa H, Nakata K (2019) Second-look arthroscopy after anatomic anterior cruciate ligament reconstruction: bone-patellar tendon-bone versus hamstring tendon graft. J Orthop Sci 24:488–493
Moher D, Shamseer L, Clarke M, Ghersi D, Liberati A, Petticrew M, Shekelle P, Stewart LA, PRISMA-P Group (2015) Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst Rev 4:1
Offerhaus C, Albers M, Nagai K, Arner JW, Hoher J, Musahl V, Fu FF (2018) Individualized anterior cruciate ligament graft matching. In vivo comparison of cross-sectional areas of hamstring, patellar, and quadriceps tendon grafts and ACL insertion area. Am J Sports Med 46:2646–2652
Park SY, Oh H, Park S, Lee JH, Lee SH, Yoon KH (2013) Factors predicting hamstring tendon autograft diameters and resulting failure rates after anterior cruciate ligament reconstruction. Knee Surg Sports Traumatol Arthrosc 21:1111–1118
Ramkumar PN, Hadley MD, Jones MH, Farrow LD (2018) Hamstring autograft in ACL reconstruction: a 13-year predictive analysis of anthropometric factors and surgeon trends relating to graft size. Orthop J Sports Med 6:2325967118779788
Rucker G, Schwarzer G, Carpenter JR, Schumacher M (2008) Undue reliance on I2 in assessing heterogeneity may mislead. BMC Med Res 8:79
Salmon LJ, Heath E, Akrawi H, Roe JP, Linklater J, Pinczewski LA (2018) 20-year outcomes of anterior cruciate ligament reconstruction with hamstring tendon autograft. The catastrophic effect of age and posterior tibial slope. Am J Sports Med 46:531–643
Sasaki N, Farraro KF, Kim KE, Woo SL-Y (2014) Biomechanical evaluation of the quadriceps tendon autograft for anterior cruciate ligament reconstruction: a cadaveric study. Am J Sports Med 42:723–730
Sheean AJ, Musahl V, Slone HS, Xerogeanes JW, Milinkovic D, Fink C, Hoser C, International Quadriceps Tendon Interest Group (2018) Quadriceps tendon autograft for arthroscopic knee ligament reconstruction: use it now, use it often. Br J Sports Med 52:698–701
Sica GT (2006) Bias in research studies. Radiology 238:780–789
Slim K, Nini E, Forester D, Kwiatkowski F, Panis Y, Chipponi J (2003) Methodological index for non-randomized studies (MINORS): development and validation of a new instrument. Anz J Surg 73:713–716
Tegner Y, Lysholm J (1985) Rating systems in the evaluation of knee ligament injuries. Clin Orthop Relat Res 198:43–49
Todd DC, Ghasem AD, Xerogeanes JW (2015) Height, weight, and age predict quadriceps tension length and thickness in skeletally immature patients. Am J Sports Med 43:945–952
Wilkerson GB, Denegar CR (2018) A growing consensus for change in interpretation of clinical research evidence. J Athl Train 53:320–326
Xerogeanes JW, Mitchell PM, Karasev PA, Kolesov IA, Romine SE (2013) Anatomic and morphological evaluation of the quadriceps tendon using 3-dimensional magnetic resonance imaging reconstruction. Applications for anterior cruciate ligament autograft choice and placement. Am J Sports Med 41:2392–2399
Acknowledgements
Thanks to Dr. Kenneth Linfield, PhD, Director of Graduate Education, Clinical Psychology Program, Spalding University, Louisville, Kentucky, USA for his statistical consultation.
Funding
There was no funding for this study.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
This manuscript is a systematic review and meta-analysis. Human participant research was not performed by any of the authors in carrying out this study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Nyland, J., Collis, P., Huffstutler, A. et al. Quadriceps tendon autograft ACL reconstruction has less pivot shift laxity and lower failure rates than hamstring tendon autografts. Knee Surg Sports Traumatol Arthrosc 28, 509–518 (2020). https://doi.org/10.1007/s00167-019-05720-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-019-05720-y