
Abstract
Introduction
The Kager fat pad is one of the largest soft tissue structures local to the ankle joint, yet it is poorly understood. It has been hypothesised to have a role in Achilles tendinopathy. This study aimed to investigate the pressure areas in the Kager fat pad adjacent to the Achilles tendon and to assess the anatomy and deformation of the Kager fat pad in cadavers.
Methods
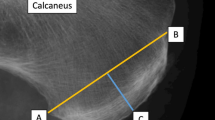
Twelve fresh frozen cadaveric ankles (mean age 44 years, range 38–51) were mounted in a customized testing rig, enabling plantar flexion and dorsiflexion of the ankle, with the Achilles tendon loaded. A needle tipped pressure sensor was inserted in two areas of the Kager fat pad under ultrasound guidance (retrocalcaneal bursa and at 3 cm proximal from Achilles insertion). Pressure readings were recorded at different flexion angles. Following testing, the specimens were dissected to expose the Kager fat pad and retrieve it for analysis. MRI images were also taken from three healthy volunteers and the Kager fat pad deformation examined.
Results
Mean pressures significantly increased in all specimens at terminal ankle plantar and dorsi flexion in both regions (p < 0.05). The Kager fat pad was consistently adherent to the Achilles at its posterior aspect for a mean length of 7.7 cm (SD 0.27, 89% of KFP length). The most distal part of the Kager fat pad was the exception and it detached from the Achilles to give way to the retroalcaneal bursa for a mean length of 0.92 cm (SD 0.24, 11% of KFP length). The bursal space is partially occupied by a constant ‘wedge’ extension of Kager fat pad. The mean volume of the whole Kager fat pad was 10.6 ml (SD 3.37). Video and MRI demonstrated that the Kager fat pad undergoes significant deformation during plantar flexion as it is displaced superiorly by the Achilles, with the wedge being forced into the retrocalcaneal bursal space.
Conclusion
The Kager fat pad does not remain static during ankle range of motion, but deforms and its pressure also changes. This observation supports the theory that it acts as a shock-absorber to the Achilles tendon and pathological changes to the fat pad may be clinically important in the development of Achilles tendinopathy.





Similar content being viewed by others


References
Webborn N, Morrissey D, Sarvananthan K, Chan O (2015) Acute tear of the fascia cruris at the attachment to the Achilles tendon: a new diagnosis. Br J Sports Med 49:1398–1403
Ward ER, Andersson G, Backman LJ, Gaida JE (2016) Fat pads adjacent to tendinopathy: more than a coincidence? Br J Sports Med 50:1491–1492
Bohnsack M, Hurschler C, Demirtas T, Rühmann O, Stukenborg-Colsman C, Wirth CJ (2005) Infrapatellar fat pad pressure and volume changes of the anterior compartment during knee motion: possible clinical consequences to the anterior knee pain syndrome. Knee Surg Sport Traumatol Arthrosc 13(2):135–141
Lohrer H, Nauck T (2014) Retrocalcaneal bursitis but not Achilles tendinopathy is characterized by increased pressure in the retrocalcaneal bursa. Clin Biomech 29:283–288
Lohrer H, Raabe T, Nauck T, Arentz S (2011) Minimally invasive retrocalcaneal bursa pressure measurement: development and pilot application. Arch Orthop Trauma Surg 131:719–723
Stephen JM, Marsland D, Masci L, Calder JDF, El Daou H (2018) Differential motion and compression between the plantaris and Achilles tendons: a contributing factor to midportion Achilles tendinopathy? Am J Sports Med 46:955–960
Roaas A, Andersson GB (1982) Normal range of motion of the hip, knee and ankle joints in male subjects, 30–40 years of age. Acta Orthop Scand 53:205–208
Rasband W ImageJ, US National Institutes of Health, Bethesda, Maryland, USA
Abràmoff MD, Magalhães PJRS (2004) Image processing with ImageJ. Biophotonics 11:36–42
Hughes SW (2005) Archimedes revisited: a faster, better, cheaper method of accurately measuring the volume of small objects. Phys Educ IOP Publ 40:468–474
Theobald P, Bydder G, Dent C, Nokes L, Pugh N, Benjamin M (2006) The functional anatomy of Kager’s fat pad in relation to retrocalcaneal problems and other hindfoot disorders. J Anat 208:91–97
De Jonge S, Van Den Berg C, De Vos RJ, Van Der Heide HJL, Weir A, Verhaar JAN, Bierma-Zeinstra SMA, Tol JL (2011) Incidence of midportion Achilles tendinopathy in the general population. Br J Sports Med 45(13):1026–1028
Józsa L, Kannus P (1997) Overuse injuries of tendons. In: Józsa L, Kannus P (eds) Human tendons: anatomy, physiology and pathology. Champaign, IL, pp 164–253
Canoso JJ (1998) The premiere enthesis. J Rheumatol 25:1254–1256
Langberg H, Skovgaard D, Bülow J, Kjaer M (1999) Negative interstitial pressure in the peritendinous region during exercise. J Appl Physiol 87:999–1002
Funding
This study was part of and was made possible thanks to the “ESSKA-AFAS Pau Golanó Research Fellowship” awarded to Francesc Malagelada by ESSKA-AFAS under the supervision of Mr James Calder at Fortius Clinic, London, UK. Further funding was provided by Fortius Research and Education Foundation, London, UK.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
This article does not contain any studies with human participants or animals performed by any of the authors.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
167_2019_5585_MOESM1_ESM.m4v
Supplementary material 1 (M4 V 18558 kb). Dissected specimen throughout the ankle range of motion. Changes in the shape of the KFP seen from ankle plantar flexion to dorsiflexion
167_2019_5585_MOESM2_ESM.avi
Supplementary material 2 (AVI 222 kb). MRI edited video. Using MRI sagital cuts of the ankle along several positions throughout the range of motion the changes in shape of the KFP can be analysed. Note the elongation and narrowing experienced by the Kager’s triangle in full dorsiflexion
Rights and permissions
About this article

Cite this article
Malagelada, F., Stephen, J., Dalmau-Pastor, M. et al. Pressure changes in the Kager fat pad at the extremes of ankle motion suggest a potential role in Achilles tendinopathy. Knee Surg Sports Traumatol Arthrosc 28, 148–154 (2020). https://doi.org/10.1007/s00167-019-05585-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-019-05585-1