
Abstract
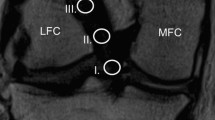
The aims of this study were to quantify the angle and placement of an anterior cruciate ligament (ACL) grafted with a single incision ACL reconstruction technique using postoperative magnetic resonance imaging (MRI), and to compare the results with those with a native ACL. Between February 1996 and May 2004, 96 consecutive patients, who had undergone postoperative MRI of the knee followed by an arthroscopically assisted ACL reconstruction with either a hamstring tendon or bone-patellar tendon-bone (BTB) autograft, were enrolled in this study. The femoral tunnel was drilled using the transtibial technique. The patients were divided into two groups; the hamstring tendon graft group (group H; 50 patients) and the BTB graft group (group B; 46 patients). All the patients including both groups in this study underwent postoperative MRI and were followed up for a minimum of 2 years. The control group (group C) consisted of 50 patients whose meniscus tear had been operated on by arthroscopy and whose ACL was intact. The orientation of the ACL ligament or graft was measured using three different methods: the sagittal ACL angle, the ACL-Blumensaat line angle, and the coronal ACL angle. The mean sagittal ACL angle in group C (58.7 ± 3.8°) was significantly lower than in groups H (64.6 ± 4.2°) and B (71.3 ± 6.0°). The mean ACL-Blumensaat line angle in group C (8.6 ± 3.6°) was also significantly lower than in groups H (12.8 ± 5.2°) and B (18.0 ± 5.3°). The mean coronal ACL angle in group C (65.9 ± 4.4°) was lower than that in groups H (73.5 ± 2.4°) and B (75.2 ± 2.9°). The grafted ACL of the hamstring tendon and BTB grafts on the postoperative MRI showed a significant vertical angle in the coronal and sagittal plane compared with the native ACL. In the sagittal plane, the hamstring tendon graft was positioned more obliquely than the BTB graft, which had a larger angle of the tibial tunnel, in an attempt to prevent a graft-tunnel mismatch. The postoperative MRI study showed that the more horizontally the angle of the tibial tunnel can be placed in a single incision ACL reconstruction, the more efficiently it can produce a graft closer to the native ACL.






Similar content being viewed by others


References
Arnold MP, Kooloos J, van Kampen A (2001) Single-incision technique misses the anatomical femoral anterior cruciate ligament insertion: a cadaver study. Knee Surg Sports Traumatol Arthrosc 9:194–199
Bach BR Jr, Tradonsky S, Bojchuk J, Levy ME, Bush-Joseph CA, Khan NH (1998) Arthroscopically assisted anterior cruciate ligament reconstruction using patellar tendon autograft. Five- to nine-year follow-up evaluation. Am J Sports Med 26:20–29
Barrett GR, Richardson K (1996) Comparison of rear-entry (two-incision) and endoscopic techniques for reconstruction of the anterior cruciate ligament. J South Orthop Assoc 5:87–95
Brown CH Jr, Sklar JH (1999) Endoscopic anterior cruciate ligamentreconstruction using doubled gracilis and semitendinosus tendons and endobutton femoral fixation. Oper Tech Sports Med 7:201–213
Cain EL Jr, Clancy WG Jr (2002) Anatomic endoscopic anterior cruciate ligament reconstruction with patella tendon autograft. Orthop Clin North Am 33:717–725
Canale ST (2003) Campbell’s operative orthopaedics, 10th edn. Mosby, Philadelphia
Corry IS, Webb JM, Clingeleffer AJ, Pinczewski LA (1999) Arthroscopic reconstruction of the anterior cruciate ligament. A comparison of patellar tendon autograft and four-strand hamstring tendon autograft. Am J Sports Med 27:444–454
Corsetti JR, Jackson DW (1996) Failure of anterior cruciate ligament reconstruction: the biologic basis. Clin Orthop Relat Res:42–49
Delay BS, Smolinski RJ, Wind WM, Bowman DS (2001) Current practices and opinions in ACL reconstruction and rehabilitation: results of a survey of the American Orthopaedic Society for Sports Medicine. Am J Knee Surg 14:85–91
Drosdowech DS, Fowler PJ (1996) Arthroscopic hamstring anteriorcruciate ligament reconstruction with endobutton femoral fixation. Oper Tech Orthopaed 6:147–151
Ejerhed L, Kartus J, Sernert N, Kohler K, Karlsson J (2003) Patellar tendon or semitendinosus tendon autografts for anterior cruciate ligament reconstruction? A prospective randomized study with a two-year follow-up. Am J Sports Med 31:19–25
Eriksson K et al (2001) A comparison of quadruple semitendinosus and patellar tendon grafts in reconstruction of the anterior cruciate ligament. J Bone Joint Surg Br 83:348–354
Frank CB, Jackson DW (1997) The science of reconstruction of the anterior cruciate ligament. J Bone Joint Surg Am 79:1556–1576
Fu FH, Benjamin C (1999) Anterior cruciate ligament reconstruction using quadruple hamstring. Oper Tech Orthopaed 9:264–272
Fu FH, Bennett CH, Ma CB, Menetrey J, Lattermann C (2000) Current trends in anterior cruciate ligament reconstruction. Part II. Operative procedures and clinical correlations. Am J Sports Med 28:124–130
Gabriel MT, Wong EK, Woo SL, Yagi M, Debski RE (2004) Distribution of in situ forces in the anterior cruciate ligament in response to rotatory loads. J Orthop Res 22:85–89
Good L, Odensten M, Gillquist J (1991) Intercondylar notch measurements with special reference to anterior cruciate ligament surgery. Clin Orthop Relat Res 263:185–189
Harner CD, Marks PH, Fu FH, Irrgang JJ, Silby MB, Mengato R (1994) Anterior cruciate ligament reconstruction: endoscopic versus two-incision technique. Arthroscopy 10:502–512
Howell SM, Clark JA, Farley TE (1991) A rationale for predicting anterior cruciate graft impingement by the intercondylar roof. A magnetic resonance imaging study. Am J Sports Med 19:276–282
Howell SM, Deutsch ML (1999) Comparison of endoscopic and two-incision techniques for reconstructing a torn anterior cruciate ligament using hamstring tendons. Arthroscopy 15:594–606
Howell SM, Gittins ME, Gottlieb JE, Traina SM, Zoellner TM (2001) The relationship between the angle of the tibial tunnel in the coronal plane and loss of flexion and anterior laxity after anterior cruciate ligament reconstruction. Am J Sports Med 29:567–574
Howell SM, Hull ML (1998) Aggressive rehabilitation using hamstring tendons: graft construct, tibial tunnel placement, fixation properties, and clinical outcome. Am J Knee Surg 11:120–127
Howell SM, Wallace MP, Hull ML, Deutsch ML (1999) Evaluation of the single-incision arthroscopic technique for anterior cruciate ligament replacement. A study of tibial tunnel placement, intraoperative graft tension, and stability. Am J Sports Med 27:284–293
Insall JN (2001) Surgery of the knee, 3rd edn, Churchill Livingstone, Philadelpia
Jackson DW, Gasser SI (1994) Tibial tunnel placement in ACL reconstruction. Arthroscopy 10:124–131
Kenna B, Simon TM, Jackson DW, Kurzweil PR (1993) Endoscopic ACL reconstruction: a technical note on tunnel length for interference fixation. Arthroscopy 9:228–230
Kleipool AE, van Loon T, Marti RK (1994) Pain after use of the central third of the patellar tendon for cruciate ligament reconstruction. 33 patients followed 2–3 years. Acta Orthop Scand 65:62–66
Kocher MS, Steadman JR, Briggs K, Zurakowski D, Sterett WI, Hawkins RJ (2002) Determinants of patient satisfaction with outcome after anterior cruciate ligament reconstruction. J Bone Joint Surg Am 84-A:1560–1572
Larson RV (1996) Anterior cruciate ligament reconstruction with hamstring tendons. Oper Tech Orthopaed 6:138–146
Lintner DM, Dewitt SE, Moseley JB (1996) Radiographic evaluation of native anterior cruciate ligament attachments and graft placement for reconstruction. A cadaveric study. Am J Sports Med 24:72–78
Loh JC, Fukuda Y, Tsuda E, Steadman RJ, Fu FH, Woo SL (2003) Knee stability and graft function following anterior cruciate ligament reconstruction: Comparison between 11 o’clock and 10 o’clock femoral tunnel placement. 2002 Richard O’Connor Award paper. Arthroscopy 19:297–304
Miller MD, Hinkin DT (1996) The “N + 7 rule” for tibial tunnel placement in endoscopic anterior cruciate ligament reconstruction. Arthroscopy 12:124–126
Mueller W (1983) The knee. Springer, Berlin
Nogalski MP, Bach BR Jr, Bush-Joseph CA, Luergans S (1995) Trends in decreased hospitalization for anterior cruciate ligament surgery: double-incision versus single-incision reconstruction. Arthroscopy 11:134–138
O’Neill DB (1996) Arthroscopically assisted reconstruction of the anterior cruciate ligament. A prospective randomized analysis of three techniques. J Bone Joint Surg Am 78:803–813
Odensten M, Gillquist J (1985) Functional anatomy of the anterior cruciate ligament and a rationale for reconstruction. J Bone Joint Surg Am 67:257–262
Olszewski AD, Miller MD, Ritchie JR (1998) Ideal tibial tunnel length for endoscopic anterior cruciate ligament reconstruction. Arthroscopy 14:9–14
Reat JF, Lintner DM (1997) One-versus two-incision ACL reconstruction. A prospective, randomized study. Am J Knee Surg 10:198–208
Sachs RA, Daniel DM, Stone ML, Garfein RF (1989) Patellofemoral problems after anterior cruciate ligament reconstruction. Am J Sports Med 17:760–765
Sakane M, Fox RJ, Woo SL, Livesay GA, Li G, Fu FH (1997) In situ forces in the anterior cruciate ligament and its bundles in response to anterior tibial loads. J Orthop Res 15:285–293
Shino K, Nakagawa S, Inoue M, Horibe S, Yoneda M (1993) Deterioration of patellofemoral articular surfaces after anterior cruciate ligament reconstruction. Am J Sports Med 21:206–211
Williams RJ III, Hyman J, Petrigliano F, Rozental T, Wickiewicz TL (2004) Anterior cruciate ligament reconstruction with a four-strand hamstring tendon autograft. J Bone Joint Surg Am 86-A:225–232
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Ahn, J.H., Lee, S.H., Yoo, J.C. et al. Measurement of the graft angles for the anterior cruciate ligament reconstruction with transtibial technique using postoperative magnetic resonance imaging in comparative study. Knee Surg Sports Traumatol Arthr 15, 1293–1300 (2007). https://doi.org/10.1007/s00167-007-0389-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-007-0389-6