
Abstract
Purpose
The best renal replacement therapy (RRT) modality remains controversial. We compared mortality and short- and long-term renal recovery between patients treated with continuous RRT and intermittent hemodialysis.
Methods
Patients of the prospective observational multicenter cohort database OUTCOMEREA™ were included if they underwent at least one RRT session between 2004 and 2014. Differences in patients’ baseline and daily characteristics between treatment groups were taken into account by using a marginal structural Cox model, allowing one to substantially reduce the bias resulting from confounding factors in observational longitudinal data analysis. The composite primary endpoint was 30-day mortality and dialysis dependency.
Results
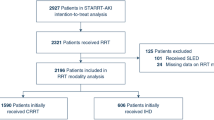
Among 1360 included patients with RRT, 544 (40.0 %) and 816 (60.0 %) were initially treated by continuous RRT and intermittent hemodialysis, respectively. At day 30, 39.6 % patients were dead. Among survivors, 23.8 % still required RRT. There was no difference between groups for the primary endpoint in global population (HR 1.00, 95 % CI 0.77–1.29; p = 0.97). In patients with higher weight gain at RRT initiation, mortality and dialysis dependency were significantly lower with continuous RRT (HR 0.54, 95 % CI 0.29–0.99; p = 0.05). Conversely, this technique appeared to be deleterious in patients without shock (HR 2.24, 95 % CI 1.24–4.04; p = 0.01). Six-month mortality and persistent renal dysfunction were not influenced by the RRT modality in patients with dialysis dependence at ICU discharge.
Conclusion
Continuous RRT did not appear to improve 30-day and 6-month patient outcomes. It seems beneficial for patients with fluid overload, but might be deleterious in the absence of hemodynamic failure.



Similar content being viewed by others
References
Clec’h C, Gonzalez F, Lautrette A, Nguile-Makao M, Garrouste-Orgeas M, Jamali S, Golgran-Toledano D, Descorps-Declere A, Chemouni F, Hamidfar-Roy R, Azoulay E, Timsit JF (2011) Multiple-center evaluation of mortality associated with acute kidney injury in critically ill patients: a competing risks analysis. Crit Care 15:R128
Clec’h C, Darmon M, Lautrette A, Chemouni F, Azoulay E, Schwebel C, Dumenil AS, Garrouste-Orgeas M, Goldgran-Toledano D, Cohen Y, Timsit JF (2012) Efficacy of renal replacement therapy in critically ill patients: a propensity analysis. Crit Care 16:R236
Gammelager H, Christiansen CF, Johansen MB, Tonnesen E, Jespersen B, Sorensen HT (2013) Five-year risk of end-stage renal disease among intensive care patients surviving dialysis-requiring acute kidney injury: a nationwide cohort study. Crit Care 17:R145
Bagshaw SM, Berthiaume LR, Delaney A, Bellomo R (2008) Continuous versus intermittent renal replacement therapy for critically ill patients with acute kidney injury: a meta-analysis. Crit Care Med 36:610–617
Rabindranath K, Adams J, Macleod AM, Muirhead N (2007) Intermittent versus continuous renal replacement therapy for acute renal failure in adults. Cochrane Database Syst Rev: CD003773
Vinsonneau C, Camus C, Combes A, Costa de Beauregard MA, Klouche K, Boulain T, Pallot JL, Chiche JD, Taupin P, Landais P, Dhainaut JF (2006) Continuous venovenous haemodiafiltration versus intermittent haemodialysis for acute renal failure in patients with multiple-organ dysfunction syndrome: a multicentre randomised trial. Lancet 368:379–385
Lins RL, Elseviers MM, Van der Niepen P, Hoste E, Malbrain ML, Damas P, Devriendt J (2009) Intermittent versus continuous renal replacement therapy for acute kidney injury patients admitted to the intensive care unit: results of a randomized clinical trial. Nephrol Dial Transplant 24:512–518
Misset B, Timsit JF, Chevret S, Renaud B, Tamion F, Carlet J (1996) A randomized cross-over comparison of the hemodynamic response to intermittent hemodialysis and continuous hemofiltration in ICU patients with acute renal failure. Intensive Care Med 22:742–746
Mehta RL, McDonald B, Gabbai FB, Pahl M, Pascual MT, Farkas A, Kaplan RM (2001) A randomized clinical trial of continuous versus intermittent dialysis for acute renal failure. Kidney Int 60:1154–1163
Gasparovic V, Filipovic-Grcic I, Merkler M, Pisl Z (2003) Continuous renal replacement therapy (CRRT) or intermittent hemodialysis (IHD)–what is the procedure of choice in critically ill patients? Ren Fail 25:855–862
Schneider AG, Bellomo R, Bagshaw SM, Glassford NJ, Lo S, Jun M, Cass A, Gallagher M (2013) Choice of renal replacement therapy modality and dialysis dependence after acute kidney injury: a systematic review and meta-analysis. Intensive Care Med 39:987–997
Wald R, Shariff SZ, Adhikari NK, Bagshaw SM, Burns KE, Friedrich JO, Garg AX, Harel Z, Kitchlu A, Ray JG (2014) The association between renal replacement therapy modality and long-term outcomes among critically ill adults with acute kidney injury: a retrospective cohort study. Crit Care Med 42:868–877
KDIGO (2011) Section 5: dialysis interventions for treatment of AKI. Kidney Int Suppl 2:89–115
Benson K, Hartz AJ (2000) A comparison of observational studies and randomized, controlled trials. N Engl J Med 342:1878–1886
Robins JM, Hernan MA, Brumback B (2000) Marginal structural models and causal inference in epidemiology. Epidemiology 11:550–560
Clec’h C, Alberti C, Vincent F, Garrouste-Orgeas M, de Lassence A, Toledano D, Azoulay E, Adrie C, Jamali S, Zaccaria I, Cohen Y, Timsit JF (2007) Tracheostomy does not improve the outcome of patients requiring prolonged mechanical ventilation: a propensity analysis. Crit Care Med 35:132–138
Uehlinger DE, Jakob SM, Ferrari P, Eichelberger M, Huynh-Do U, Marti HP, Mohaupt MG, Vogt B, Rothen HU, Regli B, Takala J, Frey FJ (2005) Comparison of continuous and intermittent renal replacement therapy for acute renal failure. Nephrol Dial Transplant 20:1630–1637
John S, Griesbach D, Baumgartel M, Weihprecht H, Schmieder RE, Geiger H (2001) Effects of continuous haemofiltration vs intermittent haemodialysis on systemic haemodynamics and splanchnic regional perfusion in septic shock patients: a prospective, randomized clinical trial. Nephrol Dial Transplant 16:320–327
Davenport A (2009) Continuous renal replacement therapies in patients with acute neurological injury. Semin Dial 22:165–168
Palevsky PM, Zhang JH, O’Connor TZ, Chertow GM, Crowley ST, Choudhury D, Finkel K, Kellum JA, Paganini E, Schein RM, Smith MW, Swanson KM, Thompson BT, Vijayan A, Watnick S, Star RA, Peduzzi P (2008) Intensity of renal support in critically ill patients with acute kidney injury. N Engl J Med 359:7–20
Bailly S, Pirracchio R, Timsit JF (2016) What’s new in the quantification of causal effects from longitudinal cohort studies: a brief introduction to marginal structural models for intensivists. Intensive Care Med 42:576–579
Hernan MA, Brumback B, Robins JM (2000) Marginal structural models to estimate the causal effect of zidovudine on the survival of HIV-positive men. Epidemiology 11:561–570
Vaara ST, Reinikainen M, Wald R, Bagshaw SM, Pettila V (2014) Timing of RRT based on the presence of conventional indications. Clin J Am Soc Nephrol 9:1577–1585
Bellomo R, Ronco C (1999) Continuous renal replacement therapy in the intensive care unit. Intensive Care Med 25:781–789
Augustine JJ, Sandy D, Seifert TH, Paganini EP (2004) A randomized controlled trial comparing intermittent with continuous dialysis in patients with ARF. Am J Kidney Dis 44:1000–1007
Schortgen F, Soubrier N, Delclaux C, Thuong M, Girou E, Brun-Buisson C, Lemaire F, Brochard L (2000) Hemodynamic tolerance of intermittent hemodialysis in critically ill patients: usefulness of practice guidelines. Am J Respir Crit Care Med 162:197–202
Grams ME, Estrella MM, Coresh J, Brower RG, Liu KD (2011) Fluid balance, diuretic use, and mortality in acute kidney injury. Clin J Am Soc Nephrol 6:966–973
Teixeira C, Garzotto F, Piccinni P, Brienza N, Iannuzzi M, Gramaticopolo S, Forfori F, Pelaia P, Rocco M, Ronco C, Anello CB, Bove T, Carlini M, Michetti V, Cruz DN (2013) Fluid balance and urine volume are independent predictors of mortality in acute kidney injury. Crit Care 17:R14
Herrler T, Tischer A, Meyer A, Feiler S, Guba M, Nowak S, Rentsch M, Bartenstein P, Hacker M, Jauch KW (2010) The intrinsic renal compartment syndrome: new perspectives in kidney transplantation. Transplantation 89:40–46
Prowle JR, Echeverri JE, Ligabo EV, Ronco C, Bellomo R (2010) Fluid balance and acute kidney injury. Nat Rev Nephrol 6:107–115
Heung M, Wolfgram DF, Kommareddi M, Hu Y, Song PX, Ojo AO (2012) Fluid overload at initiation of renal replacement therapy is associated with lack of renal recovery in patients with acute kidney injury. Nephrol Dial Transplant 27:956–961
Stoneking LR, Winkler JP, DeLuca LA, Stolz U, Stutz A, Luman JC, Gaub M, Wolk DM, Fiorello AB, Denninghoff KR (2015) Physician documentation of sepsis syndrome is associated with more aggressive treatment. West J Emerg Med 16:401–407
Yang S, Eaton CB, Lu J, Lapane KL (2014) Application of marginal structural models in pharmacoepidemiologic studies: a systematic review. Pharmacoepidemiol Drug Saf 23:560–571
Jun M, Heerspink HJ, Ninomiya T, Gallagher M, Bellomo R, Myburgh J, Finfer S, Palevsky PM, Kellum JA, Perkovic V, Cass A (2010) Intensities of renal replacement therapy in acute kidney injury: a systematic review and meta-analysis. Clin J Am Soc Nephrol 5:956–963
Van Wert R, Friedrich JO, Scales DC, Wald R, Adhikari NK (2010) High-dose renal replacement therapy for acute kidney injury: systematic review and meta-analysis. Crit Care Med 38:1360–1369
Lyndon WD, Wille KM, Tolwani AJ (2012) Solute clearance in CRRT: prescribed dose versus actual delivered dose. Nephrol Dial Transplant 27:952–956
Jun M, Bellomo R, Cass A, Gallagher M, Lo S, Lee J (2014) Timing of renal replacement therapy and patient outcomes in the randomized evaluation of normal versus augmented level of replacement therapy study. Crit Care Med 42:1756–1765
Schetz M, Gunst J, De Vlieger G, Van den Berghe G (2015) Recovery from AKI in the critically ill: potential confounders in the evaluation. Intensive Care Med 41:1648–1657
Acknowledgments
The authors thank Celine Feger, M.D. (EMIBiotech), for her editorial support.
Members of the Outcomerea Study Group
Scientific Committee: Jean-François Timsit (Medical and Infectious Diseases ICU, Bichat-Claude Bernard Hospital, Paris, France; UMR 1137 Inserm–Paris Diderot University IAME, F75018, Paris); Elie Azoulay (Medical ICU, Saint Louis Hospital, Paris, France); Maïté Garrouste-Orgeas (ICU, Saint-Joseph Hospital, Paris, France); Jean-Ralph Zahar (Infection Control Unit, Angers Hospital, Angers, France); Christophe Adrie (ICU, Delafontaine Hospital, Saint Denis, and Physiology, Cochin Hospital, Paris, France); Michael Darmon (Medical ICU, Saint Etienne University Hospital, St Etienne, France); and Christophe Clec’h (ICU, Avicenne Hospital, Bobigny, and UMR 1137 Inserm–Paris Diderot university IAME, F75018, Paris, France).
Biostatistical and Information System Expertise: Jean-Francois Timsit (Medical and Infectious Diseases ICU, Bichat-Claude Bernard Hospital, Paris, France; UMR 1137 Inserm–Paris Diderot university IAME, F75018, Paris); Corinne Alberti (Medical Computer Sciences and Biostatistics Department, Robert Debré Hospital, Paris, France); Adrien Français (Integrated Research Center U823, Grenoble, France); Aurélien Vesin (OUTCOMEREA organization and Integrated Research Center U823, Grenoble, France); Stephane Ruckly (OUTCOMEREA organization and Inserm UMR 1137 IAME, F75018, Paris); Sébastien Bailly (Grenoble University Hospital Inserm UMR 1137 IAME, F75018, Paris) and Christophe Clec’h (ICU, Avicenne Hospital, Bobigny, and Inserm UMR 1137 IAME, F75018, Paris, France); Frederik Lecorre (Supelec, France); Didier Nakache (Conservatoire National des Arts et Métiers, Paris, France); and Aurélien Vannieuwenhuyze (Tourcoing, France).
Investigators of the OUTCOMEREA Database: Christophe Adrie (ICU, Delafontaine Hospital, Saint Denis, and Physiology, Cochin Hospital, Paris, France); Bernard Allaouchiche (ICU, Pierre Benite Hospital, Lyon, France); Laurent Argaud (Medical ICU, Hospices Civils de Lyon, Lyon, France); Claire Ara-Somohano (Medical ICU, University Hospital, Grenoble, France); Elie Azoulay (Medical ICU, Saint Louis Hospital, Paris, France); Francois Barbier (medical-surgical ICU, Orleans, France), Jean-Pierre Bedos (ICU, Versailles Hospital, Versailles, France); Julien Bohé (ICU, Hôpital Pierre Benite, Lyon France), Lila Bouadma (ICU, Bichat Hospital, Paris, France); Christine Cheval (ICU, Hyeres Hospital, Hyeres, France); Christophe Clec’h (ICU, Avicenne Hospital, Bobigny, France); Michael Darmon (ICU, Saint Etienne Hospital, Saint Etienne, France); Anne-Sylvie Dumenil (Antoine Béclère Hospital, Clamart, France); Claire Dupuis (Bichat hospital and UMR 1137 Inserm–Paris Diderot University IAME, F75018, Paris, France), Marc Gainier hôpital la Timone, Marseille, France), Akim Haouache (Surgical ICU, H Mondor Hospital, Creteil, France); Samir Jamali (ICU, Dourdan, Dourdan Hospital, Dourdan, France); Hatem Khallel (ICU, Cayenne General Hospital, Cayenne, France); Alexandre Lautrette (ICU, G Montpied Hospital, Clermont-Ferrand, France); Guillaume Marcotte (Surgical ICU, Hospices Civils de Lyon, Lyon, France); Eric Le Miere (ICU, Louis Mourier Hospital, Colombes, France); Maxime Lugosi (Medical ICU, University Hospital Grenoble, Grenoble, France); Bruno Mourvillier (ICU, Bichat Hospital, Paris, France); Benoît Misset (ICU, Saint-Joseph Hospital, Paris, France); Delphine Moreau (ICU, Saint-Louis Hospital, Paris, France); Bruno Mourvillier (ICU, Bichat Hospital, Paris, France); Laurent Papazian (Hopital Nord, Marseille, France), Benjamin Planquette (pulmonology ICU, George Pompidou Hospital, Versailles, France); Bertrand Souweine (ICU, G Montpied Hospital, Clermont-Ferrand, France); Carole Schwebel (ICU, A Michallon Hospital, Grenoble, France); Gilles Troché (ICU, Antoine Béclère Hospital, Clamart, France); Marie Thuong (ICU, Delafontaine Hospital, Saint Denis, France); Guillaume Thierry (ICU, Saint-Louis Hospital, Paris, France); Dany Toledano (ICU, Gonesse Hospital, Gonesse, France); and Eric Vantalon (SICU, Saint-Joseph Hospital, Paris, France).
Study Monitors: Julien Fournier, Caroline Tournegros, Stéphanie Bagur, Mireille Adda, Vanessa Vindrieux, Loic Ferrand, Nadira Kaddour, Boris Berthe, Samir Bekkhouche, Kaouttar Mellouk, Sylvie Conrozier, Igor Theodose, Veronique Deiler, and Sophie Letrou.
Author information
Authors and Affiliations
Consortia
Corresponding author
Ethics declarations
Funding
The study was entirely funded by the OUTCOMEREA research network. AST received an educational grant from the French Kidney Foundation under the aegis of the French Medical Research Foundation; code DEA2014FDR/FRM04_FdR-SdN-SFD_FRM_TRUCHE.
Conflicts of interest
The authors declare that they have no conflict of interest.
Additional information
Take-home message: Optimal renal replacement therapy (RRT) technique in the ICU remains controversial, in patients with shock or fluid overload. Cohort studies suggested increased risk of persistent acute kidney injury or dialysis dependency with intermittent hemodialysis. In a MSM Cox model in a cohort of 1360 patients adjusted on daily patients’ characteristics, we found that RRT modality did not influenced neither 30-day mortality nor renal outcome. In subgroups, continuous RRT benefits patients with hemodynamic instability and is deleterious in patients with hemodynamic instability.
This article was presented at the 2016 congress of the French-Language Society of Intensive Care.
The members of the OUTCOMEREA Study Group are listed at the end of this article and in the electronic supplementary material (file ESM 2).
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Truche, AS., Darmon, M., Bailly, S. et al. Continuous renal replacement therapy versus intermittent hemodialysis in intensive care patients: impact on mortality and renal recovery. Intensive Care Med 42, 1408–1417 (2016). https://doi.org/10.1007/s00134-016-4404-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00134-016-4404-6