
Abstract
Purpose
Up to 38 % of children with cancer require pediatric intensive care unit (PICU) admission within 3 years of diagnosis, with reported PICU mortality of 13–27 % far exceeding that of the general PICU population. PICU outcomes data for individual cancer types are lacking and may help identify patients at risk for poor clinical outcomes.
Methods
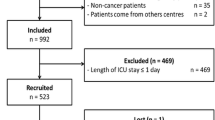
We performed a retrospective multicenter analysis of 10,365 PICU admissions of cancer patients no greater than 21 years old among 112 PICUs between 1 January 2009 and 30 June 2012. We evaluated the effect of cancer type, age, gender, genetic syndrome, stem cell transplantation, PRISM3 score, infections, and critical care interventions on PICU mortality.
Results
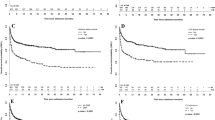
After excluding scheduled perioperative admissions, cancer patients represented 4.2 % of all PICU admissions (10,365/246,346), had overall mortality of 6.8 % (708/10,365) vs. 2.4 % (5,485/230,548) in the general PICU population (RR = 2.9, 95 % CI 2.7–3.1, p < 0.001), and accounted for 11.4 % of all PICU deaths (708/6,215). Hematologic cancer patients had greater median PRISM3 score (8 vs 2, p < 0.001), rates of sepsis (27 vs 9 %, RR = 2.9, 95 % CI 2.6–3.1, p < 0.001), and mortality (9.6 vs 4.5 %, RR = 2.1, 95 % CI 1.8–2.5, p < 0.001) compared to solid cancer patients. Among hematologic cancer patients, stem cell transplantation, diagnosis of acute myeloid leukemia, PRISM3 score, and infection were all independently associated with PICU mortality.
Conclusions
Children with cancer account for 4.2 % of PICU admissions and 11.4 % of PICU deaths. Hematologic cancer patients have significantly higher admission illness severity, rates of infections, and PICU mortality than solid cancer patients. These data may be useful in risk stratification for closer monitoring and patient counseling.



Similar content being viewed by others

References
National Cancer Institute (2014) Surveillance, epidemiology, and end results (SEER) program research data (1973-2011). DCCPS, Surveillance Res Prog, Surveillance Sys Branch. http://www.seer.cancer.gov
Dalton HJ, Slonim AD, Pollack MM (2003) Multicenter outcome of pediatric oncology patients requiring intensive care. Pediatr Hematol Oncol 20:643–649
Rosenman MB, Vik T, Hui SL, Breitfeld PP (2005) Hospital resource utilization in childhood cancer. J Pediatr Hematol Oncol 27:295–300
Pollack MM, Patel KM, Ruttimann UE (1996) PRISM III: an updated pediatric risk of mortality score. Crit Care Med 24:743–752
Tilford JM, Roberson PK, Lensing S, Fiser DH (1998) Differences in pediatric ICU mortality risk over time. Crit Care Med 26:1737–1743
Pound CM, Johnston DL, Armstrong R, Gaboury I, Menon K (2008) The morbidity and mortality of pediatric oncology patients presenting to the intensive care unit with septic shock. Pediatr Blood Cancer 51:584–588. doi:10.1002/pbc.21670
Haase R, Lieser U, Kramm C et al (2011) Management of oncology patients admitted to the paediatric intensive care unit of a general children’s hospital—a single center analysis. Klin Padiatr 223:142–146. doi:10.1055/s-0031-1275291
Meyer S, Gottschling S, Biran T, Georg T, Ehlayil K, Graf N, Gortner L (2005) Assessing the risk of mortality in paediatric cancer patients admitted to the paediatric intensive care unit: a novel risk score? Eur J Pediatr 164:563–567. doi:10.1007/s00431-005-1695-y
Owens C, Mannion D, O’Marcaigh A, Waldron M, Butler K, O’Meara A (2011) Indications for admission, treatment and improved outcome of paediatric haematology/oncology patients admitted to a tertiary paediatric ICU. Ir J Med Sci 180:85–89. doi:10.1007/s11845-010-0634-8
Hallahan AR, Shaw PJ, Rowell G, O’Connell A, Schell D, Gillis J (2000) Improved outcomes of children with malignancy admitted to a pediatric intensive care unit. Crit Care Med 28:3718–3721
van Veen A, Karstens A, van der Hoek AC, Tibboel D, Hahlen K, van der Voort E (1996) The prognosis of oncologic patients in the pediatric intensive care unit. Intensive Care Med 22:237–241
Sivan Y, Schwartz PH, Schonfeld T, Cohen IJ, Newth CJ (1991) Outcome of oncology patients in the pediatric intensive care unit. Intensive Care Med 17:11–15
Ha EJ, Kim S, Jin HS, Bae KW, Lim HJ, Seo JJ, Park SJ (2010) Early changes in SOFA score as a prognostic factor in pediatric oncology patients requiring mechanical ventilatory support. J Pediatr Hematol Oncol 32:e308–e313. doi:10.1097/MPH.0b013e3181e51338
Heying R, Schneider DT, Korholz D, Stannigel H, Lemburg P, Gobel U (2001) Efficacy and outcome of intensive care in pediatric oncologic patients. Crit Care Med 29:2276–2280
Heney D, Lewis IJ, Lockwood L, Cohen AT, Bailey CC (1992) The intensive care unit in paediatric oncology. Arch Dis Child 67:294–298
Tamburro R (2005) Pediatric cancer patients in clinical trials of sepsis: factors that predispose to sepsis and stratify outcome. Pediatr Crit Care Med 6:S87–S91. doi:10.1097/01.PCC.0000161288.00396.49
Tamburro RF, Barfield RC, Shaffer ML et al (2008) Changes in outcomes (1996–2004) for pediatric oncology and hematopoietic stem cell transplant patients requiring invasive mechanical ventilation. Pediatr Crit Care Med 9:270–277. doi:10.1097/PCC.0b013e31816c7260
Fiser RT, West NK, Bush AJ, Sillos EM, Schmidt JE, Tamburro RF (2005) Outcome of severe sepsis in pediatric oncology patients. Pediatr Crit Care Med 6:531–536
Baden L, Bensinger W, Casper C et al (2012) NCCN clinical practice guidelines in oncology: prevention and treatment of cancer-related infections. J Natl Compr Canc Netw 10:1412–1445
Haase R, Mathony U, Lieser U, Nagel F, Sitka U, Burdach S (2003) Oncology patients in a pediatric intensive care unit—a 7-year experience. Klin Padiatr 215:234–240. doi:10.1055/s-2003-41399
Dursun O, Hazar V, Karasu GT, Uygun V, Tosun O, Yesilipek A (2009) Prognostic factors in pediatric cancer patients admitted to the pediatric intensive care unit. J Pediatr Hematol Oncol 31:481–484. doi:10.1097/MPH.0b013e3181a330ef
Vogiatzi L, Ilia S, Sideri G et al (2013) Invasive candidiasis in pediatric intensive care in Greece: a nationwide study. Intensive Care Med 39:2188–2195. doi:10.1007/s00134-013-3057-y
Ben Abraham R, Toren A, Ono N, Weinbroum AA, Vardi A, Barzilay Z, Paret G (2002) Predictors of outcome in the pediatric intensive care units of children with malignancies. J Pediatr Hematol Oncol 24:23–26
Akhtar N, Fadoo Z, Panju S, Haque A (2011) Outcome and prognostic factors seen in pediatric oncology patients admitted in PICU of a developing country. Indian J Pediatr 78:969–972. doi:10.1007/s12098-011-0391-3
Singer K, Subbaiah P, Hutchinson R, Odetola F, Shanley TP (2011) Clinical course of sepsis in children with acute leukemia admitted to the pediatric intensive care unit. Pediatr Crit Care Med 12:649–654. doi:10.1097/PCC.0b013e31821927f1
Gupta P, Green JW, Tang X et al (2014) Comparison of high-frequency oscillatory ventilation and conventional mechanical ventilation in pediatric respiratory failure. JAMA Pediatr 168:243–249. doi:10.1001/jamapediatrics.2013.4463
Typpo KV, Petersen NJ, Petersen LA, Mariscalco MM (2010) Children with chronic illness return to their baseline functional status after organ dysfunction on the first day of admission in the pediatric intensive care unit. J Pediatr 157(108–113):e1. doi:10.1016/j.jpeds.2009.12.029
Typpo KV, Petersen NJ, Hallman DM, Markovitz BP, Mariscalco MM (2009) Day 1 multiple organ dysfunction syndrome is associated with poor functional outcome and mortality in the pediatric intensive care unit. Pediatr Crit Care Med 10:562–570. doi:10.1097/PCC.0b013e3181a64be1
Steliarova-Foucher E, Stiller C, Lacour B, Kaatsch P (2005) International classification of childhood cancer, third edition. Cancer 103:1457–1467. doi:10.1002/cncr.20910
Weiss SL, Parker B, Bullock ME, Swartz S, Price C, Wainwright MS, Goodman DM (2012) Defining pediatric sepsis by different criteria: discrepancies in populations and implications for clinical practice. Pediatr Crit Care Med 13:e219–e226. doi:10.1097/PCC.0b013e31823c98da
Goldstein B, Giroir B, Randolph A, International Consensus Conference on Pediatric Sepsis (2005) International pediatric sepsis consensus conference: definitions for sepsis and organ dysfunction in pediatrics. Pediatr Crit Care Med 6:2–8. doi:10.1097/01.PCC.0000149131.72248.E6
Pollack MM, Ruttimann UE, Getson PR (1988) Pediatric risk of mortality (PRISM) score. Crit Care Med 16:1110–1116
Ludbrook J, Dudley H (1994) Issues in biomedical statistics: analysing 2 × 2 tables of frequencies. Aust N Z J Surg 64:780–787
Diggle PJ, Heagerty P, Liang K, Zeger SL (2002) Analysis of longitudinal data. Oxford Statistical Science Series. Oxford University Press, Oxford
Hardin J, Hilbe J (2003) Generalized estimating equations. Chapman Hall/CRC, London
Pancera CF, Hayashi M, Fregnani JH, Negri EM, Deheinzelin D, de Camargo B (2008) Noninvasive ventilation in immunocompromised pediatric patients: eight years of experience in a pediatric oncology intensive care unit. J Pediatr Hematol Oncol 30:533–538. doi:10.1097/MPH.0b013e3181754198
Gow KW, Heiss KF, Wulkan ML et al (2009) Extracorporeal life support for support of children with malignancy and respiratory or cardiac failure: the extracorporeal life support experience. Crit Care Med 37:1308–1316. doi:10.1097/CCM.0b013e31819cf01a
Di Nardo M, Locatelli F, Palmer K et al (2014) Extracorporeal membrane oxygenation in pediatric recipients of hematopoietic stem cell transplantation: an updated analysis of the Extracorporeal Life Support Organization experience. Intensive Care Med 40:754–756. doi:10.1007/s00134-014-3240-9
Margolin JF (2011) Molecular diagnosis and risk-adjusted therapy in pediatric hematologic malignancies: a primer for pediatricians. Eur J Pediatr 170:419–425. doi:10.1007/s00431-011-1424-7
Demaret P, Pettersen G, Hubert P, Teira P, Emeriaud G (2012) The critically-ill pediatric hemato-oncology patient: epidemiology, management, and strategy of transfer to the pediatric intensive care unit. Ann Intensive Care 2:14. doi:10.1186/2110-5820-2-14
Piastra M, Fognani G, Franceschi A, “ICARO Italian Network For Intensive Care In Pediatric Oncology” (2011) Pediatric intensive care unit admission criteria for haemato-oncological patients: a basis for clinical guidelines implementation. Pediatr Rep 3:e13. doi:10.4081/pr.2011.e13
Acknowledgments
Statistical consultation was provided by John Kornak, PhD, UCSF Department of Biostatistics, and funded by the National Center for Advancing Translational Sciences, National Institutes of Health (NIH), through UCSF-CTSI Grant Number UL1 TR000004. The contents are solely the responsibility of the authors and do not necessarily represent the official views of the NIH. VPS data were provided by the VPS, LLC. No endorsement or editorial restriction of the interpretation of these data or opinions of the authors has been implied or stated. Dr. Zinter had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Conflicts of interest
There are no disclosures or conflicts of interest to report.
Author information
Authors and Affiliations
Corresponding author
Additional information
Take home message: Children with cancer account for 4.2 % of admissions and 11.4 % of all deaths among children admitted to the PICU. Children with hematologic cancer have significantly higher admission illness severity, rates of infections, and PICU mortality than children with solid cancer.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Zinter, M.S., DuBois, S.G., Spicer, A. et al. Pediatric cancer type predicts infection rate, need for critical care intervention, and mortality in the pediatric intensive care unit. Intensive Care Med 40, 1536–1544 (2014). https://doi.org/10.1007/s00134-014-3389-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00134-014-3389-2