
Abstract
Objective
We examined whether guiding therapy by an algorithm based on optimizing the global end-diastolic volume index (GEDVI) reduces the need for vasopressor and inotropic support and helps to shorten ICU stay in cardiac surgery patients.
Design and setting
Single-center clinical study with a historical control group at an university hospital.
Patients
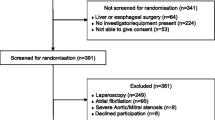
Forty cardiac bypass surgery patients were included prospectively and compared with a control group.
Interventions
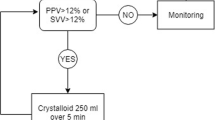
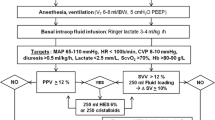
In the goal-directed therapy (GDT) group hemodynamic management was guided by an algorithm based on GEDVI. Hemodynamic goals were: GEDVI above 640 ml/m2, cardiac index above 2.5 l/min/m2, and mean arterial pressure above 70 mmHg. The control group was treated at the discretion of the attending physician based on central venous pressure, mean arterial pressure, and clinical evaluation.
Results
In the GDT group duration of catecholamine and vasopressor dependence was shorter (187 ± 70 vs. 1458 ± 197 min), and fewer vasopressors (0.73 ± 0.32 vs. 6.67 ± 1.21 mg) and catecholamines (0.01 ± 0.01 vs. 0.83 ± 0.27 mg) were administered. They received more colloids (6918 ± 242 vs. 5514 ± 171 ml). Duration of mechanical ventilation (12.6 ± 3.6 vs. 15.4 ± 4.3 h) and time until achieving status of fit for ICU discharge (25 ± 13 vs. 33 ± 17 h) was shorter in the GDT group.
Conclusions
Guiding therapy by an algorithm based on GEDVI leads to a shortened and reduced need for vasopressors, catecholamines, mechanical ventilation, and ICU therapy in patients undergoing cardiac surgery.




Similar content being viewed by others
References
Michard F, Alaya S, Zarka V, Bahloul M, Richard C, Teboul JL (2003) Global end-diastolic volume as an indicator of cardiac preload in patients with septic shock. Chest 124:1900–1908
Michard F, Teboul JL (2002) Predicting fluid responsiveness in ICU patients: a critical analysis of the evidence. Chest 121:2000–2008
Christakis GT, Fremes SE, Naylor CD, Chen E, Rao V, Goldman BS (1996) Impact of preoperative risk and perioperative morbidity on ICU stay following coronary bypass surgery. Cardiovasc Surg 4:29–35
Ryan TA, Rady MY, Bashour CA, Leventhal M, Lytle B, Starr NJ (1997) Predictors of outcome in cardiac surgical patients with prolonged intensive care stay. Chest 112:1035–1042
Weil J, Eschenhagen T, Hirt S, Magnussen O, Mittmann C, Remmers U, Scholz H (1998) Preserved Frank-Starling mechanism in human end stage heart failure. Cardiovasc Res 37:541–548
Lichtwarck-Aschoff M, Beale R, Pfeiffer UJ (1996) Central venous pressure, pulmonary artery occlusion pressure, intrathoracic blood volume, and right ventricular end-diastolic volume as indicators of cardiac preload. J Crit Care 11:180–188
Kumar A, Anel R, Bunnell E, Habet K, Zanotti S, Marshall S, Neumann A, Ali A, Cheang M, Kavinsky C, Parrillo JE (2004) Pulmonary artery occlusion pressure and central venous pressure fail to predict ventricular filling volume, cardiac performance, or the response to volume infusion in normal subjects. Crit Care Med 32:691–699
Bouchard MJ, Denault A, Couture P, Guertin MC, Babin D, Ouellet P, Carrier M, Tardif JC (2004) Poor correlation between hemodynamic and echocardiographic indexes of left ventricular performance in the operating room and intensive care unit. Crit Care Med 32:644–648
Brock H, Gabriel C, Bibl D, Necek S (2002) Monitoring intravascular volumes for postoperative volume therapy. Eur J Anaesthesiol 19:288–294
Reuter DA, Felbinger TW, Moerstedt K, Weis F, Schmidt C, Kilger E, Goetz AE (2002) Intrathoracic blood volume index measured by thermodilution for preload monitoring after cardiac surgery. J Cardiothorac Vasc Anesth 16:191–195
Reuter DA, Kirchner A, Felbinger TW, Weis FC, Kilger E, Lamm P, Goetz AE (2003) Usefulness of left ventricular stroke volume variation to assess fluid responsiveness in patients with reduced cardiac function. Crit Care Med 31:1399–1404
Katzenelson R, Perel A, Berkenstadt H, Preisman S, Kogan S, Sternik L, Segal E (2004) Accuracy of transpulmonary thermodilution versus gravimetric measurement of extravascular lung water. Crit Care Med 32:1550–1554
Fernandez-Mondejar E, Castano-Perez J, Rivera-Fernandez R, Colmenero-Ruiz M, Manzano F, Perez-Villares J, de la Chica R (2003) Quantification of lung water by transpulmonary thermodilution in normal and edematous lung. J Crit Care 18:253–258
Boussat S, Jacques T, Levy B, Laurent E, Gache A, Capellier G, Neidhardt A (2002) Intravascular volume monitoring and extravascular lung water in septic patients with pulmonary edema. Intensive Care Med 28:712–718
Sakka SG, Ruhl CC, Pfeiffer UJ, Beale R, McLuckie A, Reinhart K, Meier-Hellmann A (2000) Assessment of cardiac preload and extravascular lung water by single transpulmonary thermodilution. Intensive Care Med 26:180–187
Rivers E, Nguyen B, Havstad S, Ressler J, Muzzin A, Knoblich B, Peterson E, Tomlanovich M Early Goal-Directed Therapy Collaborative Group (2001) Early goal-directed therapy in the treatment of severe sepsis and septic shock. N Engl J Med 345:1368–1377
Gan TJ, Soppitt A, Maroof M, el-Moalem H, Robertson KM, Moretti E, Dwane P, Glass PS (2002) Goal-directed intraoperative fluid administration reduces length of hospital stay after major surgery. Anesthesiology 97:820–826
Polonen P, Ruokonen E, Hippelainen M, Poyhonen M, Takala J (2000) A prospective, randomized study of goal-oriented hemodynamic therapy in cardiac surgical patients. Anesth Analg 90:1052–1059
Goepfert MSG, Reuter DA, Akyol D, Kilger E, Goetz AE (2004) Volume management by goal directed therapy reduces catecholamine-need in cardiosurgery patients (abstract) Crit Care Med 30[Suppl 1]:588130
Combes A, Berneau JB, Luyt CE, Trouillet JL (2004) Estimation of left ventricular systolic function by single transpulmonary thermodilution. Intensive Care Med 30:1377–1383
Sakka SG, Bredle DL, Reinhart K, Meier-Hellmann A (1999) Comparison between intrathoracic blood volume and cardiac filling pressures in the early phase of hemodynamic instability of patients with sepsis or septic shock. J Crit Care 14:78–83
Sakka SG, Klein M, Reinhart K, Meier-Hellmann A (2002) Prognostic value of extravascular lung water in critically ill patients. Chest 122:2080–2086
Cheng DC, Newman MF, Duke P, Wong DT, Finegan B, Howie M, Fitch J, Bowdle TA, Hogue C, Hillel Z, Pierce E, Bukenya D (2001) The efficacy and resource utilization of remifentanil and fentanyl in fast-track coronary artery bypass graft surgery: a prospective randomized, double-blinded controlled, multi-center trial. Anesth Analg 92:1094–1102
Mythen MG, Webb AR (1994) Intra-operative gut mucosal hypoperfusion is associated with increased post-operative complications and cost. Intensive Care Med 20:99–104
Shoemaker WC, Thangathurai D, Wo CC, Kuchta K, Canas M, Sullivan MJ, Farlo J, Roffey P, Zellman V, Katz RL (1999) Intraoperative evaluation of tissue perfusion in high-risk patients by invasive and noninvasive hemodynamic monitoring. Crit Care Med 27:2147–2152
Maillet JM, Le Besnerais P, Cantoni M, Nataf P, Ruffenach A, Lessana A, Brodaty D (2003) Frequency, risk factors, and outcome of hyperlactatemia after cardiac surgery. Chest 123:1361–1366
Shoemaker WC, Patil R, Appel PL, Kram HB (1992) Hemodynamic and oxygen transport patterns for outcome prediction, therapeutic goals, and clinical algorithms to improve outcome. Feasibility of artificial intelligence to customize algorithms. Chest 102:617S–625S
Kern JW, Shoemaker WC (2002) Meta-analysis of hemodynamic optimization in high-risk patients. Crit Care Med 30:1686–1692
Shoemaker WC, Appel PL, Kram HB, Waxman K, Lee TS (1988) Prospective trial of supranormal values of survivors as therapeutic goals in high-risk surgical patients. Chest 94:1176–1186
McKendry M, McGloin H, Saberi D, Caudwell L, Brady AR, Singer M (2004) Randomised controlled trial assessing the impact of a nurse delivered, flow monitored protocol for optimisation of circulatory status after cardiac surgery. BMJ 329:258–262
Schmidlin D, Schuepbach R, Bernard E, Ecknauer E, Jenni R, Schmid ER (2001) Indications and impact of postoperative transesophageal echocardiography in cardiac surgical patients. Crit Care Med 29:2143–2148
Boldt J, Ducke M, Kumle B, Papsdorf M, Zurmeyer EL (2004) Influence of different volume replacement strategies on inflammation and endothelial activation in the elderly undergoing major abdominal surgery. Intensive Care Med 30:416–422
Pinsky MR (2002) Functional hemodynamic monitoring. Intensive Care Med 28:386–388
Wilson J, Woods I, Fawcett J, Whall R, Dibb W, Morris C, McManus E (1999) Reducing the risk of major elective surgery: randomised controlled trial of preoperative optimisation of oxygen delivery. BMJ 318:1099–1103
Acknowledgements
The authors thank the Ludwig Maximilian University Institute for Medical Data Processing, Biometry and Epidemiology for statistical support and calculation. D.A. R. a member of the Pulsion Medical Systems Medical Advisory Board and of a Medical Advisory Board of Fresenius-Kabi; he received a research grant from Pulsion Medical Systems which was not associated with the study submitted. A.E.G. is a member of the Pulsion Medical Systems Medical Advisory Board; he received no grants for this study but for experimental studies on functional hemodynamic monitoring in 1999–2000 (DM 40,000 from Pulsion Medical Systems, Germany) and no patents have been received with in relation to this study except for measurement of cerebral blood flow, together with Dr. Pfeiffer and Prof. Kübler. He personally received no payment with respect to this study; he received no additional honoraria except for travel reimbursements (from Abbott, Baxter, Fresenius Kabi, PMS).
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Rights and permissions
About this article
Cite this article
Goepfert, M.S.G., Reuter, D.A., Akyol, D. et al. Goal-directed fluid management reduces vasopressor and catecholamine use in cardiac surgery patients. Intensive Care Med 33, 96–103 (2007). https://doi.org/10.1007/s00134-006-0404-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00134-006-0404-2