
Abstract
Background
Subacromial impingement syndrome (SIS) is one of the most frequent shoulder pathologies. Initial treatment is conservative. Subacromial injection of drugs achieves a high concentration at the pathologic site with less drug use and fewer systemic side effects. Glucocorticoids are most frequently injected. One concern with steroid use is the wide array of potential systemic and local complications. Nonsteroidal anti-inflammatory drugs (NSAIDs) are also peripherally acting and can be used locally. Although intraarticular (IA) use of NSAIDs is common in orthopedic practice, it is mostly restricted to the knee joint. Reports of local NSAID for joint pathologies are relatively rare. This study compared the efficacy of single-dose subacromial injections of betamethasone and lornoxicam for treatment of SIS.
Methods
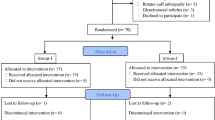
Subacromial injections of either 7.0 mg betamethasone or 8 mg lornoxicam were received by 70 patients with mean age 53 (46–68) years. Treatment outcome was assessed with Constant–Murley and UCLA questionnaires before injection and at 2‑, 4‑, and 6‑week follow-ups.
Results
The change in outcome scores compared to pretreatment was higher in the steroid group at all follow-ups (p < 0.001). Patients in the steroid group showed a significant improvement at all follow-ups compared to pretreatment (p <0.001) and previous follow-ups (p <0.05) at all times. Patients in the lornoxicam group showed a significant functional improvement in week 2 (p <0.001), which was not evident in the following weeks (p >0.05). Although functional recovery halted after week 2, outcome scores remained significantly higher than the pretreatment values at all weeks (p <0.001).
Conclusion
Although a single subacromial lornoxicam injection provides rapid functional recovery, which partially extends into the intermediate term, its results are inferior to betamethasone and it may be an alternative only in patients where corticosteroids are contraindicated.
Zusammenfassung
Hintergrund
Das subakromiale Impingementsyndrom (SIS) ist eine der häufigsten Erkrankungen der Schulter. Initial wird es konservativ behandelt. Mit der subakromialen Injektion von Medikamenten lässt sich bei geringerem Medikamenteneinsatz und weniger systemischen Nebenwirkungen eine hohe Konzentration am Ort der Erkrankung erzielen. Glukokortikoide werden am häufigsten injiziert. Bei Verwendung von Steroiden ist das große Spektrum potenzieller systemischer und lokaler Komplikationen zu bedenken. Nichtsteroidale Antirheumatika (NSAR) wirken auch peripher und können lokal eingesetzt werden. Die intraartikuläre Injektion von NSAR ist in der orthopädischen Praxis zwar üblich, aber zumeist auf das Kniegelenk beschränkt. Berichte über lokale NSAR bei Gelenkerkrankungen sind relativ selten. In der vorliegenden Studie wurde die Wirksamkeit von subakromialen Injektionen einer Einzeldosis Betamethason und Lornoxicam zur Therapie des SIS verglichen.
Methoden
Eine subakromiale Injektion entweder von 7,0 mg Betamethason oder 8 mg Lornoxicam erhielten 70 Patienten mit einem Durchschnittsalter von 53 (46–68) Jahren. Das Therapieergebnis wurde mit den Fragebögen nach Constant-Murley und UCLA (University of California, Los Angeles) vor der Injektion und bei Nachuntersuchungen nach 2, 4, und 6 Wochen ermittelt.
Ergebnisse
Die Veränderung der Therapiewerte im Vergleich zum Zustand vor der Therapie war in der Steroidgruppe bei allen Nachuntersuchungen größer (p <0,001). Bei den Patienten in der Steroidgruppe bestand eine signifikante Verbesserung in allen Nachuntersuchungen gegenüber dem Zustand vor Therapie (p <0,001) und vorherigen Nachuntersuchungen (p <0,05) zu allen Zeitpunkten. Die Patienten in der Lornoxicamgruppe zeigten eine signifikante funktionelle Verbesserung in Woche 2 (p <0,001), die sich in den folgenden Wochen nicht belegen ließ (p >0,05). Bei ihnen kam die funktionelle Besserung nach Woche 2 zwar zu einem Stillstand, aber die Therapiewerte blieben signifikant höher als die Werte vor Therapie in sämtlichen Wochen (p <0,001).
Schlussfolgerung
Obwohl eine einzelne subakromiale Lornoxicaminjektion zu einer schnellen funktionellen Besserung führt, die sich teilweise bis in den mittelfristigen Bereich erstreckt, sind die Ergebnisse dieser Therapie der Gabe von Betamethason unterlegen und stellen möglicherweise eine Alternative nur für Patienten dar, bei denen Kortikosteroide kontraindiziert sind.
Similar content being viewed by others


References
van der Sande R, Rinkel WD, Gebremariam L, Hay EM, Koes BW, Huisstede BM (2013) Subacromial impingement syndrome: Effectiveness of pharmaceutical interventions-nonsteroidal anti-inflammatory drugs, corticosteroid, or other injections: A systematic review. Arch Phys Med Rehabil 94:961–976
Çelik D, Atalar AC, Güçlü A, Demirhan M (2009) The contribution of subacromial injection to the conservative treatment of impingement syndrome. Acta Orthop Traumatol Turc 43:331–335
Akgün K, Birtane M, Akarirmak U (2004) Is local subacromial corticosteroid injection beneficial in subacromial impingement syndrome? Clin Rheumatol 23:496–500
Rømsing J, Møiniche S, Ostergaard D, Dahl JB (2000) Local infiltration with NSAIDs for postoperative analgesia: evidence for a peripheral analgesic action. Acta Anaesthesiol Scand 44:672–683
Young A, Buvanendran A (2011) Multimodal systemic and intra-articular analgesics. Int Anesthesiol Clin 49:117–133
Talu GK, Ozyalçin S, Koltka K, Ertürk E, Akinci O, Aşik M, Pembeci K (2002) Comparison of efficacy of intraarticular application of tenoxicam, bupivacaine and tenoxicam: Bupivacaine combination in arthroscopic knee surgery. Knee Surg Sports Traumatol Arthrosc 10:355–360
Arroll B, Goodyear-Smith F (2005) Corticosteroid injections for painful shoulder: A meta-analysis. Br J Gen Pract 55:224–228
Alvarez CM, Litchfield R, Jackowski D, Griffin S, Kirkley A (2005) A prospective, double-blind, randomized clinical trial comparing subacromial injection of betamethasone and xylocaine to xylocaine alone in chronic rotator cuff tendinosis. Am J Sports Med 33:255–262
Koester MC, Dunn WR, Kuhn JE, Spindler KP (2007) The efficacy of subacromial corticosteroid injection in the treatment of rotator cuff disease: A systematic review. J Am Acad Orthop Surg 15:3–11
Dogu B, Yucel SD, Sag SY, Bankaoglu M, Kuran B (2012) Blind or ultrasound-guided corticosteroid injections and short-term response in subacromial impingement syndrome: A randomized, double-blind, prospective study. Am J Phys Med Rehabil 91:658–665
Buchbinder R, Green S, Youd JM (2003) Corticosteroid injections for shoulder pain. Cochrane Database Syst Rev 1:CD004016
Coombes BK, Bisset L, Vicenzino B (2010) Efficacy and safety of corticosteroid injections and other injections for management of tendinopathy: A systematic review of randomised controlled trials. Lancet 376:1751–1767
Karthikeyan S, Kwong HT, Upadhyay PK, Parsons N, Drew SJ, Griffin D (2010) A double-blind randomised controlled study comparing subacromial injection of tenoxicam or methylprednisolone in patients with subacromial impingement. J Bone Joint Surg Br 92:77–82
Saricaoglu F, Dal D, Atilla P, Iskit AB, Tarhan O, Aşan E, Aypar UA (2008) Effect of intraarticular injection of lornoxicam on the articular cartilage & synovium in rat. Indian J Med Res 127:362–365
Alagöl A, Calpur OU, Usar PS, Turan N, Pamukcu Z (2005) Intraarticular analgesia after arthroscopic knee surgery: Comparison of neostigmine, clonidine, tenoxicam, morphine and bupivacaine. Knee Surg Sports Traumatol Arthrosc 13:658–663
Jacobson E, Assareh H, Cannerfelt R, Renström P, Jakobsson J (2006) Pain after elective arthroscopy of the knee: A prospective, randomised, study comparing conventional NSAID to coxib. Knee Surg Sports Traumatol Arthrosc 14:1166–1170
Lee SC, Rha DW, Chang WH (2011) Rapid analgesic onset of intra-articular hyaluronic acid with ketorolac in osteoarthritis of the knee. J Back Musculoskelet Rehabil 24:31–38
Stålman A, Tsai JA, Segerdahl M, Dungner E, Arner P, Felländer-Tsai L (2009) Ketorolac but not morphine exerts inflammatory and metabolic effects in synovial membrane after knee arthroscopy: A double-blind randomized prospective study using the microdialysis technique. Reg Anesth Pain Med 34:557–564
Itzkowitch D, Ginsberg F, Leon M, Bernard V, Appelboom T (1996) Peri-articular injection of tenoxicam for painful shoulders: A double-blind, placebo controlled trial. Clin Rheumatol 15:604–609
Schroeder S, Heuser A, Tellmann A, Goebel KJ, Woehrmann T (2012) Local tolerance of intraarticular administration of lornoxicam into the rabbit knee joint. Rheumatol Int 32:2661–2667
Koltka K, Koknel-Talu G, Asik M, Ozyalcin S (2011) Comparison of efficacy of intraarticular application of magnesium, levobupivacaine and lornoxicam with placebo in arthroscopic surgery. Knee Surg Sports Traumatol Arthrosc 19:1884–1889
Ersan Ö, Akkaya T, Arık E, Ateş Y (2012) Intra-articular levobupivacaine, lornoxicam and morphine analgesia after knee arthroscopy: A randomized, controlled trial. Acta Orthop Traumatol Turc 46:411–415
Beaudreuil J, Nizard R, Thomas T, Peyre M, Liotard JP, Boileau P, Marc T, Dromard C, Steyer E, Bardin T, Orcel P, Walch G (2009) Contribution of clinical tests to the diagnosis of rotator cuff disease: A systematic literature review. Joint Bone Spine 76:15–19
Joo JH, Park JW, Kim JS, Kim YH (2011) Is intra-articular multimodal drug injection effective in pain management after total knee arthroplasty? A randomized, double-blinded, prospective study. J Arthroplasty 26:1095–1099
Rosseland LA, Helgesen KG, Breivik H, Stubhaug A (2004) Moderate-to-severe pain after knee arthroscopy is relieved by intraarticular saline: A randomized controlled trial. Anesth Analg 98:1546–1551
Petri M, Dobrow R, Neiman R, Whiting-O’Keefe Q, Seaman WE (1987) Randomized, double-blind, placebo-controlled study of the treatment of the painful shoulder. Arthritis Rheum 30:1040–1045
Rhon DI, Boyles RB, Cleland JA (2014) One-year outcome of subacromial corticosteroid injection compared with manual physical therapy for the management of the unilateral shoulder impingement syndrome: A pragmatic randomized trial. Ann Intern Med 161:161–169
Min KS, St Pierre P, Ryan PM, Marchant BG, Wilson CJ, Arrington ED (2013) A double-blind randomized controlled trial comparing the effects of subacromial injection with corticosteroid versus NSAID in patients with shoulder impingement syndrome. J Shoulder Elbow Surg 22:595–601
Habib GS, Saliba W, Nashashibi M (2010) Local effects of intra-articular corticosteroids. Clin Rheumatol 29:347–356
Salerno A, Hermann R (2006) Efficacy and safety of steroid use for postoperative pain relief. Update and review of the medical literature. J Bone Joint Surg Am 88:1361–1372
Habib G, Jabbour A, Artul S, Hakim G (2014) Intra-articular methylprednisolone acetate injection at the knee joint and the hypothalamic-pituitary-adrenal axis: A randomized controlled study. Clin Rheumatol 33:99–103
Muto T, Kokubu T, Mifune Y, Inui A, Harada Y, Takase F, Kuroda R, Kurosaka M (2014) Temporary inductions of matrix metalloprotease-3 (MMP-3) expression and cell apoptosis are associated with tendon degeneration or rupture after corticosteroid injection. J Orthop Res 32:1297–1304
Mikolyzk DK, Wei AS, Tonino P, Marra G, Williams DA, Himes RD, Wezeman FH, Callaci JJ (2009) Effect of corticosteroids on the biomechanical strength of rat rotator cuff tendon. J Bone Joint Surg Am 91:1172–1180
Haraldsson BT, Langberg H, Aagaard P, Zuurmond AM, van El B, Degroot J, Kjaer M, Magnusson SP (2006) Corticosteroids reduce the tensile strength of isolated collagen fascicles. Am J Sports Med 34:1992–1997
Hamano H, Motomiya M, Iwasaki N (2013) Adverse effect of repeated corticosteroid injections for trigger finger on flexor pulley system. J Hand Surg Eur Vol 38:326–327
Chen SK, Lu CC, Chou PH, Guo LY, Wu WL (2009) Patellar tendon ruptures in weight lifters after local steroid injections. Arch Orthop Trauma Surg 129:369–372
Fitzgerald BT, Hofmeister EP, Fan RA, Thompson MA (2005) Delayed flexor digitorum superficialis and profundus ruptures in a trigger finger after a steroid injection: A case report. J Hand Surg Am 30:479–482
Ozyuvaci H, Bilgic B, Ozyuvaci E, Altan A, Altug T, Karaca C (2004) Intra-articular injection of tenoxicam in rats: Assessment of the local effects on the articular cartilage and synovium. J Int Med Res 32:312–316
Dogan N, Erdem AF, Gundogdu C, Kursad H, Kizilkaya M (2004) The effects of ketorolac and morphine on articular cartilage and synovium in the rabbit knee joint. Can J Physiol Pharmacol 82:502–505
Riggin CN, Tucker JJ, Soslowsky LJ, Kuntz AF (2014) Intra-articular tibiofemoral injection of a nonsteroidal anti-inflammatory drug has no detrimental effects on joint mechanics in a rat model. J Orthop Res 32:1512–1519
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
M. Aksakal, C. Ermutlu, G. Özkaya, and Y. Özkan declare that they have no competing interests.
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Informed consent was obtained from all individual participants included in the study.
Additional information
Authors’ contribution C. Ermutlu designed the study and drafted the manuscript. M. Aksakal performed the interventions, collected data, and participated in drafting the manuscript. G. Özkaya participated in design of the study and performed the statistical analysis. Y. Özkan conceived the study, participated in its design and coordination, and helped to draft the manuscript. All authors read and approved the final manuscript.
Rights and permissions
About this article

Cite this article
Aksakal, M., Ermutlu, C., Özkaya, G. et al. Lornoxicam injection is inferior to betamethasone in the treatment of subacromial impingement syndrome. Orthopäde 46, 179–185 (2017). https://doi.org/10.1007/s00132-016-3302-5
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00132-016-3302-5