
Abstract
Purpose
Mental health problems are prevalent after combat; they are also common in its absence. Estimates of deployment-attributability vary. This paper quantifies the contribution of different subtypes of occupational trauma to post-deployment mental health problems.
Methods
Participants were a cohort of 16,193 Canadian personnel undergoing post-deployment mental health screening after return from the mission in Afghanistan. The screening questionnaire assessed post-traumatic stress disorder, depression, panic disorder, generalized anxiety disorder, and exposure to 30 potentially traumatic deployment experiences. Logistic regression estimated adjusted population attributable fractions (PAFs) for deployment-related trauma, which was treated as count variables divided into several subtypes of experiences based on earlier factor analytic work.
Results
The overall PAF for overall deployment-related trauma exposure was 57.5% (95% confidence interval 44.1, 67.7) for the aggregate outcome of any of the four assessed problems. Substantial PAFs were seen even at lower levels of exposure. Among subtypes of trauma, exposure to a dangerous environment (e.g., receiving small arms fire) and to the dead and injured (e.g., handling or uncovering human remains) had the largest PAFs. Active combat (e.g., calling in fire on the enemy) did not have a significant PAF.
Conclusions
Military deployments involving exposure to a dangerous environment or to the dead or injured will have substantial impacts on mental health in military personnel and others exposed to similar occupational trauma. Potential explanations for divergent findings in the literature on the extent to which deployment-related trauma contributes to the burden of mental disorders are discussed.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Post-deployment mental health problems occur in many who have deployed to the conflicts in southwest Asia [1, 2]. For example, 13.5% of Canadian Armed Forces personnel who deployed in support of the mission in Afghanistan were diagnosed with a mental disorder that was attributed to their deployment [2]. Mental health problems are strongly associated with outcomes of interest to any employer, including absenteeism [3,4,5], decreased productivity [3, 6, 7], long-term disability [8], and unwanted turnover [8, 9]. Mental health services represent a large and growing fraction of the health services delivered by military organizations [10].
Post-deployment mental health problems are driven by both military factors (such as combat exposure) and non-military factors (such as gender [11], child abuse [12, 13], and past mental health [11]). Of deployment-related factors, exposure to potentially traumatic deployment experiences has the strongest and most consistent relationship to post-deployment mental health problems [1, 14,15,16].
There is considerable variation in estimates among studies that have explored the relationship between combat and mental health, even within studies of deployments to similar conflict area over the same time frame. A review of the association of combat exposure and mental health in non-treatment seeking populations identified 53 studies in which estimates of PTSD prevalence ranged from 0 to 48%, depression ranged from 4 to 45%, and substance misuse ranged from 4 to 66% [14] among persons who served in the armed forces during the Iraq and Afghanistan conflicts.
Few studies have directly quantified the contribution of combat experiences to the burden of mental health problems, and estimates vary widely. For example, in 2002, the population attributable fraction (PAF) in Canadian military personnel for combat or peacekeeping with respect to any past-year mental disorder was 6% in women and 9% for men [17]. There were sizable PAFs only for past-year PTSD (47% in men, 24% in women); PAFs for depression were not statistically significant [17]. In 2013, similar survey data showed that the PAF for deployment in support of the CAF’s mission in Afghanistan with respect to any past-year mental disorder was remarkably similar (9% in a largely male sample); child abuse victimization, however, had a much greater PAF (29%) [13].
General population data from the US showed an apparently greater contribution of combat: The PAF for the US adult population as a whole was 27% for past-year PTSD and 7% for past-year depression [18]. A recent Canadian study also found a substantial contribution, with three-quarters of personnel diagnosed with a mental disorder after return from deployment in support of the mission in Afghanistan having a condition deemed to be deployment-related by their clinician [2]. Consistent with this finding, modern Canadian veterans overwhelmingly attribute their mental health problems to their military service [2, 18, 19]. In contrast, emerging research findings from the US Army showing high rates of mental disorders in recruits and in personnel who had never deployed [20,21,22] have pointed controversially [23] to a powerful contribution of factors other than occupational trauma.
These findings do not readily cohere, and each has important limitations, including crude measures of occupational trauma exposure [14, 15, 17, 24], using data that pre-dated the large-scale deployments to southwest Asia since 2001 [17], failure to account for determinants of mental health other than occupational trauma [2], and use of suboptimal civilian comparison groups [25]. It has been well-documented that different specific combat experiences are differentially traumatogenic [26, 27], but few studies [17] have attempted to quantify the differential contribution of different subtypes of occupational trauma to the burden of mental health problems. Some studies have explored differences in the strength of association between specific combat experiences [27,28,29], but odds ratios are not optimal metrics for understanding the contribution of such experiences to the burden of post-deployment mental health problems, given that they do not account for the significant differences in the prevalence of the experiences. In addition, there are many potentially traumatic events during deployments [30], so looking a constrained subgroup of these [31] may underestimate the contribution of deployment-related trauma to mental health problems.
A better understanding of the relative contribution of types of combat experiences to mental health problems would help military organizations, other high-risk employers [32], and veteran services providers predict mental disorder burden in future operations. Understanding which types of experiences contribute most to the burden of illness may also inform training practices, which may have protective effects against trauma-related psychopathology [33].
Hence, this paper uses data collected from military personnel in the context of post-deployment mental health screening to estimate the overall and trauma subtype-specific PAFs for post-deployment mental health problems.
Methods
Study participants
Participants were 16,193 Canadian Armed Forces (CAF) personnel who underwent Enhanced Post-deployment Screening over the period 1 January 2009 through 1 July 2012 following deployment in support of the CAF’s mission in Afghanistan. Personnel fulfilled a broad range of roles in various locations in Southwest Asia: Army personnel largely deployed to Kandahar Province (Afghanistan) in combat and combat support roles, Navy personnel to ships in the Arabian Gulf, and Air Force personnel to an air base in the United Arab Emirates [34]. The vast majority of the 158 CAF fatalities occurred in Army personnel in Kandahar Province.
The screening process
Screening is required 90–180 days post-deployment for personnel who deploy overseas for 60 days or more. The process consists of completion of a self-report health questionnaire followed by a personal interview with a mental health clinician.
Notwithstanding the policy requirement for screening, non-compliance does occur, though compliance with questionnaire completion is at least 76% [11], with this being calculated by dividing the number of screening questionnaires received relative to the number of personnel identified as requiring the screening, using administrative data. This represents a lower limit to compliance because screenings that cannot be matched to a given deployment due to missing data are considered non-compliant. Limitations in our data sources do not facilitate exploration of differences in the characteristics of those who do and do not complete the screenings.
Questionnaire content
Sociodemographic and military characteristics
These were assessed using a series of items developed for the screening process, including: age, sex, first official language, education, marital status, years of military service, rank, component (Regular, compared with Reserve Force), and element (Army, Navy, or Air Force) [11].
Potentially traumatic deployment experiences
These were assessed using a 30-item combat exposure scale [35], adapted from the US Army’s Walter Reed Institute for Research Combat Experiences Scale [36]. Each item was a yes/no question assessing whether the experience had ever occurred over the most recent deployment. The total exposure score reflected the sum of the positive responses to these 30 items.
Three subscales representing the simple sum of positive responses to constituent items were calculated, with the items for each subscale being identified using principal components analysis performed using the same dataset [35]. The first factor, “dangerous environment”, (12 items, explaining 63.8% of variance, Cronbach’s α = 0.9) reflected dangers inherent in the combat environment, including exposure to small arms fire, improvised explosive devices, and hostile civilians. “Exposure to the dead and injured” (7 items, 7.6% of variance, α = 0.8) reflected exposures to human remains, death, and unit casualties. “Active combat” (5 items, 5.7% of variance, α = 0.7) represented exposure to combat activities and included 5 items such as receiving sniper fire and directing fire at the enemy. A fourth factor (4.8% of variance, α = 0.3) grouped 3 items (engaging in hand-to-hand combat, feeling directly responsible for the death of a non-combatant, and feeling directly responsible for the death of a Canadian or ally personnel), titled “perceived responsibility”, was treated as a dichotomous exposure (that is, exposed to 1 or more of these 3 experiences vs. none of them) because of the observed low reliability. Two additional items (being injured and having experienced a “close call”) that cross-loaded on several factors were treated as single, dichotomous items in the analysis.
Mental health problems
Post-traumatic stress disorder (PTSD) symptoms over the previous 4 weeks were assessed using the patient checklist for PTSD, Civilian Version (PCL-C) [37] (range 17–85), using a cut-off score of 50 or higher. Major depression over the past 2 weeks and generalized anxiety disorder (GAD) over the past month were assessed using the PRIME-MD Patient Health Questionnaire (PHQ), using the developer’s recommended algorithm for “major depressive syndrome” and “other anxiety syndrome”, respectively [38]. Panic disorder in the previous month was also assessed using the PHQ, though the minimum number of symptoms criterion (4 out of 11) for the last panic attack was not imposed [11], meaning that the criterion was met if they had had a self-described anxiety or panic attack in the previous 4 weeks, if they had also had previous attacks, if they had had at least some such attacks “out of the blue”, and if they found the attacks bothersome/worrisome. A composite variable reflecting the presence of 1 or more of the preceding 4 problems was also created.
Analysis
To simplify the analysis and interpretation of results, only the first screening questionnaire was used for personnel who completed more than 1 screening over this period (n = 972). All analysis was completed using Stata, version 13.0.
Outcomes
The primary outcome was the PAF for any mental health problem for overall exposure to all 30 potentially traumatic deployment experiences. Secondary outcomes included PAFs for each of the 4 specific problems assessed, as well as the PAFs for the 6 exposure subtypes. Exploration of exposure- and disorder-specific PAFs was undertaken based on evidence of differential effects in earlier work [17].
Association of combat exposure with mental health problems
The unadjusted association between trauma, mental health problems, and potential confounders identified in earlier work [11] (age, sex, education, rank, military branch, years of military service, regular force status, and marital status) was assessed using logistic regression. Combat exposures and potential confounders having a univariate relationship with any problem (P < 0.05) were included in multivariate logistic regression models, which were used to calculate PAFs. However, to facilitate comparability and simplify reporting of results, the same control variables were included in all models. Results are expressed as adjusted odds ratios with corresponding 95% confidence intervals (CIs). All tests for statistical significance are two-sided.
Missing data
The fraction of missing sociodemographic and military characteristics was 0.4% or less. Mental health problem status was missing for between 0.5% (for PTSD) and 2.1% (for GAD). Exposure data were missing for at most 0.1% for each exposure item. Listwise deletion was used during analysis, resulting in final models containing complete data for at least 15,084 (93%) of participants.
Calculation of PAFs
PAFs were calculated using the punaf command in Stata [39]. This method used logistic regression to produce risk ratios for the exposures to calculate the PAF and CIs using the logs of two scenario means, the baseline scenario and a counterfactual scenario of no exposure. All PAFs were adjusted for potentially confounding sociodemographic and military characteristics; PAFs looking at specific exposure subtypes were adjusted for all other exposure subtypes.
For the three exposure subscales, level of exposure was collapsed into four categories representing high, medium, low, and no exposure. Cut-offs were determined pragmatically by dividing subscale scores by 3, to produce levels representing a relatively equal number of count categories per level. Multilevel PAFs were calculated using exposure subtypes as categorical variables in the logistic regression, using the approach detailed by Hanley [40]. Adjusted odds ratios, PAFs and 95% CIs were calculated and reported for each level of exposure.
Results
Sociodemographic and military characteristics
The majority of the 16,193 respondents were male, regular force, non-commissioned members under the age of 35; most were married or in a common-law relationship, served in the Army, and had not completed a university degree (Table 1).
Exposure to deployment-related trauma
14,442 (89%) were exposed to at least 1 potentially traumatic deployment experience, with the median number of experiences being 6 (interquartile range 2–12). As shown in Table 2, the most commonly reported combat exposure items were “Receiving incoming artillery, rocket or mortar fire” (63%), “Improvised explosive device (IED)/booby trap exploded near you” (60%), and “Having hostile reactions from civilians” (59%). 12,719 (79%) were exposed to 1 or more “dangerous environment” item, 11,256 (70%) were exposed to at least 1 “active combat” item, 10,751 (66%) were exposed to at least 1 “dead and injured” item, 1657 (10%) experienced a “close call”, 1235 (8%) were injured, and 783 (5%) endorsed 1 or more “perceived responsibility” item. Virtually all exposures had a significant unadjusted relationship with key outcomes, with OR ranging from 1.61 to 7.57 for PTSD and from 1.15 to 3.51 for any mental health problem (Table 2).
Mental health problems and their correlates
Approximately 6.5% of respondents reported 1 or more mental health problem, with 3.2% of respondents being above the cut-off for major depression, 2.8% for PTSD, 1.9% for GAD, and 1.8% for panic disorder. The association of any problem with sociodemographic and military characteristics is shown in Table 1. The odds of any problem differed significantly across age, sex, education, rank, branch, years of military service, regular force status, and marital status variables. Therefore, all of these correlates were included in the regression models.
Table 3 shows the adjusted ORs for the association of the overall exposure to deployment-related trauma and its subtypes with the aggregate outcome of any problem. Overall trauma exposure had a clear dose–response relationship with any problem, with the adjusted odds ratio for the most highly exposed being 9.33 (CI 6.37, 13.69) and for the least exposed, 1.93 (CI 1.42, 2.63), relative to those with no exposure. Trauma subtypes had weaker relationships with any problem, with the largest adjusted odds ratio being for perceived responsibility (2.72, CI 2.20, 3.37). Active combat was the only subtype that did not have an independent association with the aggregate outcome across all levels of exposure.
PAFs
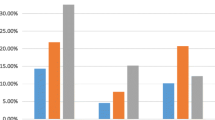
The multi-level summed PAF for overall exposure to trauma and the aggregate outcome of any problem was 57.5% (CI 44.1, 67.7; Fig. 1). The dose–response relationship seen in the adjusted OR for trauma was mirrored in the PAFs (Table 2). In the most heavily exposed group, the PAF was 87.0% (CI 81.5, 90.8), and while the PAF for the least exposed group was lower (46.7%, CI 28.3, 60.3), it still demonstrated an important contribution of trauma to the burden of mental health problems even at relatively low levels of exposure. Exposure to dangerous environment and to the dead and injured had meaningful PAFs of 32.5% (CI 16.6, 45.3) and 27.3% (CI 16.1, 37.1), respectively. Small but statistically significant PAFs were seen for low prevalence experiences (having had a close call, having been injured, or having endorsed 1 or more of the perceived responsibility items). The PAF for active combat was not statistically significant. Overall exposure for trauma had significant PAFs for all 4 problems (Fig. 2), with the largest PAF being for PTSD (84.0%, CI 69.8, 91.5) and the lowest for GAD (42.2%, CI 9.7, 63.0); however, the confidence intervals for the PAFs for different problems overlapped substantially.

Population attributable fractions by combat exposure subtype for any mental health problem. ENV dangerous environment, DEA exposure to the dead and injured, CBT active combat, CLC close call, INJ injured, RES perceived responsibility

Population attributable fraction for overall combat exposure and specific mental health problems. PTSD post-traumatic stress disorder, Panic panic disorder, GAD generalized anxiety disorder
Discussion
Summary of key findings
The primary purpose of this paper was to provide an estimate of the contribution of deployment-related trauma to the burden of mental health problems in Canadian military personnel, using a precise and detailed measure of potentially traumatic experiences. We found that overall exposure to the 30 experiences accounted for a large portion of the burden of the aggregate outcome of any mental health problem (PAF of 57.5%, CI 44.1, 67.7). The PAFs for overall trauma exposure for each specific problem were all significant, with the highest PAF being seen for PTSD (84.0%, CI 69.8, 91.5) and the lowest for GAD (42.2%, CI 9.7, 63.0). A significant contribution of deployment-related trauma was seen even in those with lower levels of exposure (e.g., the PAF for the low exposure group was still 46.7%, CI 28.3, 60.3 for the aggregate outcome of any problem). Exposure to a dangerous environment and to the dead and injured accounted for most of the burden of illness; active combat per se did not account for a statistically significant fraction.
Comparison with other findings
The other risk factors we identified for post-deployment mental health problems (e.g., female gender, not being an officer) mirror those of other research [2, 11, 41]. Prior to our research, the best evidence of the relative impact of combat exposures on mental health was limited to the estimates associated with the sum of all types of combat experiences [14, 15, 24, 42,43,44,45,46] or the relative contributions of various types of lifetime exposures [17, 42]. Grouping all combat experiences together for analysis does not allow for the separation of nuances of exposures associated with different combat roles and missions. Our findings on the contribution of exposure to the dead and injured and to a dangerous environment to the burden of mental health problems cohere with the findings of others demonstrating that these are prevalent experiences with a strong association with mental health outcomes [28, 30, 47, 48].
With respect to our primary finding, we will limit our discussion to Canadian studies on attributability, which will remove many sources of variability that may make it difficult to discern a pattern in the findings. The primary point of comparison for the present study is Sareen et al. [17] analysis of 2002 Canadian military survey data, which showed that the PAF for combat or peacekeeping on an aggregate outcome of any past-year mental disorder for the CAF as a whole was 9% in men and 6% in women [17]—well below those in the present analysis.
While there are important methodological differences between that study and the present one, the magnitude of difference in 2002 vs. over the period of the present study (2009–2012) suggests that greater combat exposure is likely an important factor in the higher PAF we documented relative to 2002 (before the mission in Afghanistan). Indeed, significant increases in combat exposure for the CAF as a whole occurred over the period 2002–2013 [41]; it would be hard to imagine that this would have no impact on its PAF. Another potential explanation is that Sareen et al. [17] did not explore the contribution of other items on the trauma inventory used in the survey that might have occurred on deployment, including items on exposure to atrocities, being in a serious accident, being threatened by a weapon, and others. The result of these omissions is that Sareen et al. [17] approach to measurement of deployment-related trauma will result in systematic underestimation of its true PAF.
This observation is nuanced by a recent finding using 2013 survey data [13] in which the PAF for participation in the mission in Afghanistan (which had occurred in 46% of respondents) with respect to any past-year disorder was only 9% for the CAF as a whole; the PAF for child abuse victimization was much greater (29%). A key difference relative to the present finding is that PAF pertains to the CAF population as a whole as opposed to the just the deployed population (in the case of the present findings). Another key difference is our inability to adjust for child abuse victimization, which is plausibly correlated with later deployment-related trauma. We also suspect that the timing of assessment is a key difference (3–6 months post-deployment) vs. more than 5-year post-deployment, on average, in the 2013 survey. Mental disorders (particularly when service-related) often lead to personnel being found unfit for continued service [19], which depletes those with service-related problems from the serving population, exerting downward pressure on PAFs for deployment-related trauma. This same mechanism likely contributed to the relatively low PAF seen in 2002 [17].
Another point of comparison for our findings is Boulos and Zamorski’s analysis of deployment-related mental disorders in a large cohort of personnel who deployed in support of the mission in Afghanistan over the period 2001–2008 [2]. That study used diagnoses and clinician attributions of their relationship with deployment that were abstracted from medical records. In 74% of those diagnosed with a post-deployment disorder, 1 or more of the disorders were judged to be related to a previous deployment (largely Afghanistan-related ones). While this approach to attribution (clinical judgement at the level of the individual patient) is clearly different from the epidemiological approach used in PAF calculations, this figure is only slightly above the PAFs for trauma and any problem noted in the present study (57%). An additional point of comparison using clinical attributions is a report featuring an analysis of similar Canadian EPDS data on an earlier cohort of Afghanistan mission-deployed personnel, using the clinician’s impression of the relationship between what they perceived to be “major concerns” identified during the screening to the most recent deployment. For major concerns on PTSD and on depression, 84 and 68% (respectively) of those screened had their major concern attributed to the most recent deployment [49]. These comparisons point to differences in the means of attribution (clinical vs. epidemiological) as being one contributor to differences in the extent of attributability of mental health problems to deployment-related trauma.
We thus tentatively offer at least five potential explanations for divergent findings in the literature as to how much of the burden of mental health problems in Canadian military personnel is accounted for by military occupational trauma:
-
1.
True differences in the extent of trauma exposure in a given military population;
-
2.
Differences in the subpopulation in which the contribution of deployment-related trauma is assessed (i.e., the deployed population vs. the entire military population);
-
3.
Systematic underestimation in studies that did not include an exhaustive list of potential deployment-related traumas;
-
4.
Differences in the timing of assessment relative to return from deployment (with selective attrition of those with mental disorders being a major mechanism for this); and
-
5.
Differences between clinical and epidemiological approaches to attribution.
Other factors may also be at play, including technical ones related to the assessment tools used, the other covariates (such as child abuse victimization) that are adjusted for in the models, and the context of the assessment (clinical screening vs. a mental health survey).
Strengths and limitations
The primary strength of this study is that it quantified the contribution of deployment-related trauma to the burden of mental health problems—an under-researched issue. The short period between return from deployment and assessment of trauma and mental health problems is another strength, minimizing the potential bias of differential release of personnel with deployment-related mental disorders [50]. We used an inventory of 30 traumatic experiences (grouped empirically using principal components analysis) and used a multi-level approach to calculation of PAFs. The primary strength of the present analysis over Boulos and Zamorski [2] approach is our use of an epidemiological as opposed to clinical approach to determination of attribution.
This study does have limitations: the assessment of mental disorders was confidential, but not anonymous, which likely led to systematic under-reporting of symptoms [51], and we were unable to assess the extent of possible participation bias. Second, we could not control for some potential confounders or effect modifiers, such as past mental health [11], childhood adversity [52], other lifetime trauma, unit cohesion, deployment length, leadership, and homecoming experiences. Third, we used cross-sectional data, which has clear limitations when it comes to establishing causality; this approach has however been used in other similar research [17, 18]. Interpretation of PAFs requires that the exposures be causal and that relevant confounders are taken into account. This assumption is particularly problematic given that prevalence, unlike incidence, is not a true measure of etiological risk; it depends on many other factors that we did not measure, such as the duration of disorder episodes [53]. There is, however, substantial evidence from longitudinal studies for the etiological role of combat in mental health problems [54, 55]. Finally, we assessed mental health problems at a single point in time. Over time, the PAF could increase or decrease.
Public health implications
Deployment-related trauma contributed significantly to the overall burden of mental disorders in this large cohort of Canadian military personnel who deployed in support of the mission in Afghanistan. Deployment of large numbers of personnel on similar operations will thus increase the overall burden of mental illness in military organizations. This has obvious implications for military organizations and for veterans’ service providers. The differential contribution of different subtypes of combat exposure permits inferences about the impact of other types of military missions or other activities with similar exposure to trauma. The two factors that contributed most heavily to the burden of mental health problems (exposure to a dangerous environment and to the dead and injured) are likely to occur on other missions. Such non-combat missions are thus expected to still contribute significantly to the overall burden of mental illness.
The meaningful PAFs even at low levels of exposure to dangerous environment and exposure to the dead and injured suggests that even those deployed to lower threat areas may see meaningful increases in the burden of mental illness; this is consistent with the non-trivial incidence of deployment-related mental disorders seen in low-threat areas in other work [2]. That is, we have identified contributions both of exposure type and of exposure dose within a given type of exposure. Our findings suggest that the large proportion of disorders that are clinically attributed to deployment is due to a genuine increase in the overall burden of mental illness and not to simple shifts in attribution for disorders that would have occurred even in the absence of deployment.
These findings also have implications for research. Replication of our findings in other populations and using other methods would be informative, given the paucity of similar studies and their discrepant results. Specific exploration of the reasons underlying the mismatch between findings on deployment trauma attributability would be valuable. Our data did not permit exploration of the psychological mechanisms underlying the differential effects of different subtypes of combat exposure on mental health problems; this is an avenue for research that could lead to more effective prevention. Exploration of the differential effects of trauma subtypes on specific mental disorders may lead to a deeper understanding of their pathogenesis. We had hoped to be able to explore this, but our dataset proved to have inadequate power leading to overly broad confidence intervals for disorder- and trauma subtype-specific PAF estimates.
Conclusion
Exposure to occupational trauma contributes significantly to the overall burden of mental health problems in Canadian military personnel who deployed in support of the mission in Afghanistan. Substantial contributions are seen at low levels of exposure, and active combat contributes very little, if at all. Hence, meaningful impacts on mental health are likely even in non-combat operations and even in personnel with low levels of exposure. Military organizations, other high-risk employers, and veterans’ services providers need to be prepared for these realities, even as Western involvement in hostilities in Southwest Asia winds down.
Abbreviations
- CAF:
-
Canadian Armed Forces
- CI:
-
Confidence interval
- EPDS:
-
Enhanced post-deployment screening
- GAD:
-
Generalized anxiety disorder
- IED:
-
Improvised explosive device
- PAF:
-
Population attributable fraction
- PHQ:
-
PRIME-MD Patient Health Questionnaire
- PTSD:
-
Post-traumatic stress disorder
- US:
-
United States of America
References
Kok BC, Herrell RK, Thomas JL, Hoge CW (2012) Posttraumatic stress disorder associated with combat service in Iraq or Afghanistan: reconciling prevalence differences between studies. J Nerv Ment Dis 200:444–450
Boulos DL, Zamorski MA (2013) Deployment-related mental disorders in Canadian Forces personnel deployed in support of the mission in Afghanistan, 2001–2008. CMAJ 185:E545–E552
De Graaf R, Tuithof M, Van Dorsselaer S, Ten Have M (2012) Comparing the effects on work performance of mental and physical disorders. Soc Psychiatry Psychiatr Epidemiol 47:1873–1883
Alonso J, Petukhova M, Vilagut G, Chatterji S, Heeringa S, Ustun TB, Alhamzawi AO, Viana MC, Angermeyer M, Bromet E, Bruffaerts R, de Girolamo G, Florescu S, Gureje O, Haro JM, Hinkov H, Hu CY, Karam EG, Kovess V, Levinson D, Medina-Mora ME, Nakamura Y, Ormel J, Posada-Villa J, Sagar R, Scott KM, Tsang A, Williams DR, Kessler RC (2011) Days out of role due to common physical and mental conditions: results from the WHO World Mental Health surveys. Mol Psychiatry 16:1234–1246
Hoge CW, Terhakopian A, Castro CA, Messer SC, Engel CC (2007) Association of posttraumatic stress disorder with somatic symptoms, health care visits, and absenteeism among Iraq war veterans. Am J Psychiatry 164:150–153
Esposito E, Wang JL, Williams JV, Patten SB (2007) Mood and anxiety disorders, the association with presenteeism in employed members of a general population sample. Epidemiol Psichiatr Soc 16:231–237
Thomas JL, Wilk JE, Riviere LA, McGurk D, Castro CA, Hoge CW (2010) Prevalence of mental health problems and functional impairment among active component and National Guard soldiers 3 and 12 months following combat in Iraq. Arch Gen Psychiatry 67:614–623
The Conference Board of Canada (2012) Mental health issues in the labour force: reducing the economic impact on Canada. The Conference Board of Canada, Ottawa
Hoge CW, Auchterlonie JL, Milliken CS (2006) Mental health problems, use of mental health services, and attrition from military service after returning from deployment to Iraq or Afghanistan. JAMA 295:1023–1032
Armed Forces Health Surveillance Center (2010) Absolute and relative morbidity burdens attributable to various illnesses and injuries, US Armed Forces, 2009. MSMR 17, pp 16–21
Zamorski MA, Rusu C, Garber BG (2014) Prevalence and correlates of mental health problems in Canadian Forces personnel who deployed in support of the mission in Afghanistan: findings from postdeployment screenings, 2009–2012. Can J Psychiatry 59:319–326
Turner S, Taillieu T, Cheung K, Zamorski M, Boulos D, Sareen J, Afifi TO (2017) Child abuse experiences and perceived need for care and mental health service use among members of the Canadian Armed Forces. Can J Psychiatry 62:413–421
Boulos D, Zamorski MA (2016) Contribution of the mission in Afghanistan to the burden of past-year mental disorders in Canadian Armed Forces personnel, 2013. Can J Psychiatry 61:64S–76S
Ramchand R, Schell TL, Karney BR, Osilla KC, Burns RM, Caldarone LB (2010) Disparate prevalence estimates of PTSD among service members who served in Iraq and Afghanistan: possible explanations. J Trauma Stress 23:59–68
Richardson LK, Frueh BC, Acierno R (2010) Prevalence estimates of combat-related post-traumatic stress disorder: critical review. Aust N Z J Psychiatry 44:4–19
Dohrenwend BP, Turner JB, Turse NA, Adams BG, Koenen KC, Marshall R (2006) The psychological risks of Vietnam for US veterans: a revisit with new data and methods. Science 313:979–982
Sareen J, Belik SL, Afifi TO, Asmundson GJ, Cox BJ, Stein MB (2008) Canadian military personnel’s population attributable fractions of mental disorders and mental health service use associated with combat and peacekeeping operations. Am J Public Health 98:2191–2198
Prigerson HG, Maciejewski PK, Rosenheck RA (2002) Population attributable fractions of psychiatric disorders and behavioral outcomes associated with combat exposure among US men. Am J Public Health 92:59–63
Boulos D, Zamorski MA (2016) Military occupational outcomes in Canadian Armed Forces personnel with and without deployment-related mental disorders. Can J Psychiatry 61:348–357
Kessler RC, Heeringa SG, Stein MB, Colpe LJ, Fullerton CS, Hwang I, Naifeh JA, Nock MK, Petukhova M, Sampson NA, Schoenbaum M, Zaslavsky AM, Ursano RJ (2014) Thirty-day prevalence of DSM-IV mental disorders among nondeployed soldiers in the US Army: results from the Army Study to Assess Risk and Resilience in Service members (Army STARRS). JAMA Psychiatry 71:504–513
Nock MK, Stein MB, Heeringa SG, Ursano RJ, Colpe LJ, Fullerton CS, Hwang I, Naifeh JA, Sampson NA, Schoenbaum M, Zaslavsky AM, Kessler RC (2014) Prevalence and correlates of suicidal behavior among soldiers: results from the Army Study to Assess Risk and Resilience in Servicemembers (Army STARRS). JAMA Psychiatry 71:514–522
Schoenbaum M, Kessler RC, Gilman SE, Colpe LJ, Heeringa SG, Stein MB, Ursano RJ, Cox KL (2014) Predictors of suicide and accident death in the Army Study to Assess Risk and Resilience in Servicemembers (Army STARRS): results from the Army Study to Assess Risk and Resilience in Service members (Army STARRS). JAMA Psychiatry 71:493–503
Hoge CW, Warner CH, Castro CA (2014) Mental health and the army. JAMA Psychiatry 71:965–966
Cesur R, Sabia JJ, Tekin E (2013) The psychological costs of war: military combat and mental health. J Health Econ 32:51–65
Gadermann AM, Gilman SE, McLaughlin KA, Nock MK, Petukhova M, Sampson NA, Kessler RC (2012) Projected rates of psychological disorders and suicidality among soldiers based on simulations of matched general population data. Mil Med 177:1002–1010
Watkins K, Sudom KA, Zamorski MA (2016) Association of combat experiences with post-traumatic stress disorder among Canadian military personnel deployed in support of the mission in Afghanistan. Mil Behav Health 4:285–292
Rona RJ, Hooper R, Jones M, Iversen AC, Hull L, Murphy D, Hotopf M, Wessely S (2009) The contribution of prior psychological symptoms and combat exposure to post Iraq deployment mental health in the UK military. J Trauma Stress 22:11–19
Iversen AC, Fear NT, Ehlers A, Hacker Hughes JG, Hull L, Earnshaw M, Greenberg N, Rona R, Wessely S, Hotopf M (2008) Risk factors for post-traumatic stress disorder among UK Armed Forces personnel. Psychol Med 38:511–522
Belik SL, Stein MB, Asmundson GJ, Sareen J (2009) Relation between traumatic events and suicide attempts in Canadian military personnel. Can J Psychiatry 54:93–104
Watkins K (2014) Deployment stressors: a review of the literature and implications for members of the Canadian Armed Forces. Res Mil 4:1–28
Sareen J, Cox BJ, Afifi TO, Stein MB, Belik SL, Meadows G, Asmundson GJ (2007) Combat and peacekeeping operations in relation to prevalence of mental disorders and perceived need for mental health care: findings from a large representative sample of military personnel. Arch Gen Psychiatry 64:843–852
de Terte I, Stephens C (2014) Psychological resilience of workers in high-risk occupations. Stress Health 30:353–355
Office of the Surgeon General UAMC (2008) Mental Health Advisory Team (MHAT) V: operation Iraqi Freedom 06–08 (Iraq); operation enduring freedom 8 (Afghanistan). US Army Medical Command, Washington, DC, pp 1–233
Zamorski MA, Boulos DL (2014) The impact of the military mission in Afghanistan on mental health in the Canadian Armed Forces: a summary of research findings. Eur J Psychotraumatol 5:23822
Sudom KA, Watkins K, Zamorski MA (2016) Stressors experienced during deployment among Canadian Armed Forces personnel: factor structure of two combat exposure scales. Mil Psychol 28:285–295
Guyker WM, Donnelly K, Donnelly JP, Dunnam M, Warner GC, Kittleson J, Bradshaw CB, Alt M, Meier ST (2013) Dimensionality, reliability, and validity of the combat experiences scale. Mil Med 178:377–384
Weathers FW, Litz BT, Huska JA, Keane TM (1994) The PTSD Checklist (PCL)--Civilian version. National Center for PTSD, Behavioral Science Division, Boston
Spitzer RL, Kroenke K, Williams JB (1999) Validation and utility of a self-report version of PRIME-MD: the PHQ primary care study. Primary care evaluation of mental disorders. Patient Health Quest JAMA 282:1737–1744
Newsom RB (2013) Attributable and unattributable risks and fractions and other scenario comparisons. STATA J 13:672–698
Hanley JA (2001) A heuristic approach to the formulas for population attributable fraction. J Epidemiol Commun Health 55:508–514
Zamorski MA, Bennett RE, Rusu C, Weeks M, Boulos D, Garber BG (2016) Prevalence of past-year mental disorders in the Canadian Armed Forces, 2002–2013. Can J Psychiatry 61:56S–63S
Erickson J, Kinley DJ, Afifi TO, Zamorski MA, Pietrzak RH, Stein MB, Sareen J (2015) Epidemiology of generalized anxiety disorder in Canadian military personnel. J Mil Vet Fam Health 1:26–36
Sundin J, Fear NT, Iversen A, Rona RJ, Wessely S (2010) PTSD after deployment to Iraq: conflicting rates, conflicting claims. Psychol Med 40:367–382
Sipos ML, Bar-Haim Y, Abend R, Adler AB, Bliese PD (2014) Postdeployment threat-related attention bias interacts with combat exposure to account for PTSD and anxiety symptoms in soldiers. Depress Anxiety 31:124–129
Sundin J, Herrell RK, Hoge CW, Fear NT, Adler AB, Greenberg N, Riviere LA, Thomas JL, Wessely S, Bliese PD (2014) Mental health outcomes in US and UK military personnel returning from Iraq. Br J Psychiatry 204:200–207
Bryan CJ, Hernandez AM, Allison S, Clemans T (2013) Combat exposure and suicide risk in two samples of military personnel. J Clin Psychol 69:64–77
Booth-Kewley S, Larson GE, Highfill-McRoy RM, Garland CF, Gaskin TA (2010) Correlates of posttraumatic stress disorder symptoms in Marines back from war. J Trauma Stress 23:69–77
Xue C, Ge Y, Tang B, Liu Y, Kang P, Wang M, Zhang L (2015) A meta-analysis of risk factors for combat-related PTSD among military personnel and veterans. PLoS One 10:e0120270
Zamorski MA (2011) Report on the findings of the enhanced post-deployment screening of those returning from Op ARCHER/Task Force Afghanistan as of 11 February 2011. Department of National Defence, Ottawa
Brunet A, Monson E, Liu A, Fikretoglu D (2015) Trauma exposure and posttraumatic stress disorders in the Canadian military. Can J Psychiatry 60:488–496
Warner CH, Appenzeller GN, Grieger T, Belenkiy S, Breitbach J, Parker J, Warner CM, Hoge C (2011) Importance of anonymity to encourage honest reporting in mental health screening after combat deployment. Arch Gen Psychiatry 68:1065–1071
Sareen J, Henriksen CA, Bolton SL, Afifi TO, Stein MB, Asmundson GJ (2013) Adverse childhood experiences in relation to mood and anxiety disorders in a population-based sample of active military personnel. Psychol Med 43:1–12
Patten S (2016) Mental health in the Canadian Armed Forces: new data, new answers and new questions
Smith TC, Ryan MA, Wingard DL, Slymen DJ, Sallis JF, Kritz-Silverstein D (2008) New onset and persistent symptoms of post-traumatic stress disorder self reported after deployment and combat exposures: prospective population based US military cohort study. BMJ 336:366–371
Wells TS, Leardmann CA, Fortuna SO, Smith B, Smith TC, Ryan MA, Boyko EJ, Blazer D (2010) A prospective study of depression following combat deployment in support of the wars in Iraq and Afghanistan. Am J Public Health 100:90–99
Acknowledgements
This research was supported via salary support from the Department of National Defence (Canada) and via additional support from the Surgeon General’s Health Research Program. The authors would like to thank Dr. Corneliu Rusu who assisted with data acquisition and cleaning.
Author information
Authors and Affiliations
Contributions
The first author developed the concept for the paper and its analytical strategy, did all data analysis, drafted the Methods and Results sections, contributed to the Introduction and Discussion, and contributed to interpretation of the findings. The second author refined the concept and analytical strategy, drafted most of the Introduction and Discussion sections, and contributed to the interpretation of the findings. Both authors edited and approved the final manuscript.
Corresponding author
Ethics declarations
Human participant protection
This study was approved by Veritas IRB (Dorval, QC) in accordance with Canada’s Tri-council Policy Statement: Ethical Conduct for Research Involving Humans (2010).
Disclaimer
The opinions expressed in this paper reflect those of the authors alone and do not represent the official policy or position of the Department of National Defence, the Canadian Armed Forces, or the Government of Canada.
Conflict of interest
On behalf of all authors, the corresponding author states that there is no conflict of interest.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Born, J.A., Zamorski, M.A. Contribution of traumatic deployment experiences to the burden of mental health problems in Canadian Armed Forces personnel: exploration of population attributable fractions. Soc Psychiatry Psychiatr Epidemiol 54, 145–156 (2019). https://doi.org/10.1007/s00127-018-1562-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00127-018-1562-6