
Summary.
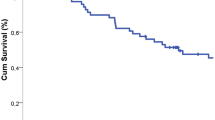
Residual tumor (R1) was proven at the proximal bronchial resection margin in 88 (3.6 %) of 2464 cases of lung cancer following lung resection and standard lymph node dissection. Postoperative complications (8 %) were: fistula of the bronchial suture line (n = 7), bleeding (n = 2) and heart luxation (n = 1). The in-hospital mortality was 16.6 %. Causes of death were: bronchial fistula (n = 7), erosion of the pulmonary artery (n = 4), respiratory failure (n = 1), and empyema (n = 1). Forty-three patients received postoperative radiation therapy. Median survival of all patients following incomplete resection was 16 months, compared to 37 months following complete resection (P < 0.001). Length of survival was independent of tumor stage, histology, site of infiltration and postoperative radiation. In conclusion, in resection for lung cancer clear margins should be verified by intraoperative frozen section. In the case of residual tumor at the bronchial resection margin, wider resection is mandatory in stage I and II if the patient meets the functional criteria. Even in stage III a and III b prognosis is significantly better after complete resection than R1-resection; the difference, however, is smaller than in lower stages.
Zusammenfassung.
Nach Lungenresektion und ipsilateraler Lymphknotendissektion wegen Bronchialcarcinoms verblieb in 88 von 2464 Fällen (3,6 %) mikroskopisch Residualtumor (R1) am zentralen Bronchusresektionsrand. Sieben Patienten entwickelten eine Insuffizienz der Bronchusnaht, 2 weitere eine Nachblutung bzw. eine Herzluxation (Morbidität 8,0 %). Die Hospitalletalität betrug 16,6 %. Todesursachen waren Bronchusnahtinsuffizienz (n = 7), Arrosionsblutung (n = 4), respiratorische Insuffizienz (n = 1) und Pleuraempyem (n = 1). Eine postoperative Bestrahlung wurde bei 43 Patienten durchgeführt. Die mediane Überlebenszeit aller Patienten nach R1-Resektion war 16 Monate gegenüber 37 Monaten nach R0-Resektion (p < 0,001). Die Überlebenszeit war unabhängig von Tumorstadium und -histologie, Lokalisation des Residualtumors in der Bronchuswand und einer Nachbestrahlung. Inkomplette Resektionen sind durch intraoperativen Schnellschnitt zu verifizieren. Sofern funktionell vertretbar, sollte in den Stadien I und II eine Nachresektion (R0) angestrebt werden; auch in den Stadien III a und III b ist bei R0-Resektion ein statistisch signifikanter Überlebensvorteil gegenüber R1-Resektion zu verzeichnen, jedoch weniger deutlich als in niedrigeren Stadien.
Similar content being viewed by others


Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Dienemann, H., Trainer, C., Hoffmann, H. et al. Inkomplette Resektionen bei Bronchialcarcinom: Morbidität und Prognose. Chirurg 68, 1014–1019 (1997). https://doi.org/10.1007/s001040050313
Published:
Issue Date:
DOI: https://doi.org/10.1007/s001040050313