
Abstract
Objective
Changes in respiratory parameters and pulmonary function tests were evaluated after shoulder arthroscopic surgery with brachial plexus block (BPB). The purpose of this study was to identify the mechanism of respiratory dysfunction after this type of surgery.
Methods
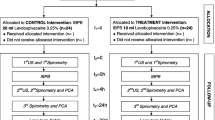
Patients undergoing arthroscopic rotator cuff repair under general anesthesia (GA) with BPB were enrolled in the arthroscopy group (n = 30) while those undergoing open reduction of a clavicle or humerus fracture under GA were enrolled in the control group (n = 30). Forced vital capacity (FVC) and forced expiratory volume 1 s (FEV1) were measured at the outpatient clinic stage (#1) before (#2) and 20 min after BPB (#3) and 1 h after extubation (#4). Respiratory variable measurements along with the cuff leak test were performed 5 min after surgical positioning (T1) and at the start of skin closure (T2). Respiratory discomfort was evaluated after extubation. The upper airway diameters and soft tissue depth of chest wall were also measured by ultrasonography at stages #3 and #4.
Results
Static compliance decreased significantly at T2 in the arthroscopy group (50 ± 11 at T1 vs. 44 ± 9 ml/cm H2O at T2, p =0.035) but not in the control group. The incidence of positive cuff leak tests at T2 was significantly higher in the arthroscopy group than in the control group (47% in the arthroscopy group vs. 17% in controls, p =0.010). While FEV1 and FVC remained stable at stages #1 and #2, FVC and FEV1 decreased at stages #3 and #4 only in the arthroscopy group (FVC in arthroscopy group, #2: 3.26 ± 0.77 l; #3: 2.55 ± 0.63 l, p =0.015 vs. #2; #4: 2.66 ± 0.41 l, p =0.040 vs. #2). The subglottic diameter decreased at #4 in the arthroscopy group, while no changes occurred in the control group (0.70 ± 0.21 cm vs. 0.85 ± 0.23 cm in the arthroscopy and control groups, respectively, p =0.011). Depth of skin to pleura increased at both intercostal spaces 1–2 and 3–4 in the arthroscopy group. There were three cases of hypoxia (SpO2 < 95%) with room air in the arthroscopy group while none occurred in the controls.
Conclusion
Shoulder arthroscopic surgery under GA with BPB induced both restrictive and obstructive pathologies. It is important to maintain a high level of awareness for the potential negative respiratory effects of this surgery especially for subjects with pre-existing cardiopulmonary disease. The measurements in this study would be useful to monitor the risk of respiratory dysfunction in these patients.
Zusammenfassung
Ziel
Evaluiert wurden die Veränderungen von atemwegsbezogenen Parametern und Lungenfunktionsuntersuchungen nach unter Plexus-brachialis-Blockade (PBB) durchgeführten arthroskopischen Operationen an der Schulter. Ziel war die Identifizierung der Mechanismen, die postoperativen Atemdysfunktionen zugrunde liegen.
Methoden
Patienten mit arthroskopischer Rotatorenmanschettenrevision in Allgemeinanästhesie (GA) und PBB wurden in die Arthroskopiegruppe (n=30) aufgenommen, Patienten mit offen behandelter Klavikula- oder Humerusfraktur in die Kontrollgruppe (n=30). Die forcierte Vitalkapazität (FVC) und das forcierte exspiratorische Einsekundenvolumen (FEV1) wurden präoperativ im ambulanten Setting (#1), vor (#2) und 20 min nach der PBB (#3) sowie 1 h nach Extubation (#4) bestimmt. Die Messung atemwegsbezogener Variablen sowie der „Cuff-leak“-Test wurden 5 min nach Lagerung (T1) und zu Beginn des Hautverschlusses (T2) durchgeführt. Atemwegsbezogene Beschwerden wurden nach der Extubation bewertet, ferner wurden zu den Messzeitpunkten #3 und #4 die Durchmesser der oberen Atemwege sowie die Weichgewebetiefe des Brustkorbs sonographisch bestimmt.
Ergebnisse
Die statische Compliance verringerte sich signifikant zum Zeitpunkt T2 in der Arthroskopiegruppe (50±11 bei T1 vs. 44±9 ml/cm H2O bei T2, p=0,035), nicht jedoch in der Kontrollgruppe. Die Inzidenz eines positiven Cuff-leak-Tests zum Zeitpunkt T2 war in der Arthroskopiegruppe signifikant höher als in der Kontrollgruppe (47 vs. 17%; p=0,010). Während FEV1/FVC erhalten blieb, verringerten sich FVC und FEV1 zu den Zeitpunkten #3 and #4 nur in der Arthroskopiegruppe [FVC in der Arthroskopiegruppe, #2: 3,26±0,77 l; #3: 2,55±0,63 l (p=0,015 vs. #2); #4: 2,66±0,41 l (p=0,040 vs. #2)]. Der subglottische Durchmesser war zum Zeitpunkt #4 in der Arthroskopiegruppe verringert, in der Kontrollgruppe dagegen unverändert (0,70±0,21 vs. 0,85±0,23 cm; p=0,011). Die Distanz zwischen Haut und Pleura, gemessen in den Interkostalräumen 1–2 und 3–4, erhöhte sich in der Arthroskopiegruppe. Anders als in der Kontrollgruppe kam es in der Arthroskopiegruppe in 3 Fällen zu einer Hypoxie [pulsoxymetrisch gemessene Sauerstoffsättigung (SpO2) <95%] unter Raumluft.
Schlussfolgerung
Bei arthroskopischen Schulteroperationen unter GA mit PBB wurden restriktive und obstruktive pathologische Veränderungen induziert. Wichtig ist ein kontinuierliches, ausgeprägtes Bewusstsein für potenzielle negative Auswirkungen dieser Operationen auf die Atmung, besonders bei Patienten mit einer vorbestehenden kardiopulmonalen Erkrankung. Die in der vorliegenden Studie vorgestellten Maßnahmen könnten beim Monitoring des atemwegsbezogenen Risikos für diese Patienten hilfreich sein.




Similar content being viewed by others


References
Berjano P, Gonzalez BG, Olmedo JF et al (1998) Complications in arthroscopic shoulder surgery. Arthroscopy 14:785–788
Orebaugh SL (2003) Life-threatening airway edema resulting from prolonged shoulder arthroscopy. Anesthesiology 99:1456–1458
Plit ML, Chhajed PN, Macdonald P et al (2002) Bilateral vocal cord palsy following interscalene brachial plexus nerve block. Anaesth Intensive Care 30:499–501
Saeki N, Kawamoto M (2011) Tracheal obstruction caused by fluid extravasation during shoulder arthroscopy. Anaesth Intensive Care 39:317–318
Hynson JM, Tung A, Guevara JE et al (1993) Complete airway obstruction during arthroscopic shoulder surgery. Anesth Analg 76:875–878
Blumenthal S, Nadig M, Gerber C et al (2003) Severe airway obstruction during arthroscopic shoulder surgery. Anesthesiology 99:1455–1456
Yoshimura E, Yano T, Ichinose K et al (2005) Airway obstruction involving a laryngeal mask airway during arthroscopic shoulder surgery. J Anesth 19:325–327
Lee JH, Cho SH, Kim SH et al (2011) Ropivacaine for ultrasound-guided interscalene block: 5 mL provides similar analgesia but less phrenic nerve paralysis than 10 mL. Can J Anaesth 58:1001–1006
Venkat G, Moon YL, Na WC et al (2009) Upper airway compromise by extravasated fluid: a rare complication after arthroscopic repair of atrophic cuff tear. Orthopedics 32. doi: 10.3928/01477447-20090818-32
De Wachter J, Van Glabbeek F, Van Riet R et al (2005) Surrounding soft tissue pressure during shoulder arthroscopy. Acta Orthop Belg 71:521–527
Gaus P, Heb B, Tanyay Z et al (2011) Epidural malpositioning of an interscalene plexus catheter. Anaesthesist 60:850–853
Walter M, Rogalla P, Spies C et al (2005) Intrathecal misplacement of an interscalene plexus catheter. Anaesthesist 54:215–219
Urmey WF, McDonald M (1992) Hemidiaphragmatic paresis during interscalene brachial plexus block: effects on pulmonary function and chest wall mechanics. Anesth Analg 74:352–357
Urmey WF, Talts KH, Sharrock NE (1991) One hundred percent incidence of hemidiaphragmatic paresis associated with interscalene brachial plexus anesthesia as diagnosed by ultrasonography. Anesth Analg 72:498–503
Wilson WC, Benumof JL (2005) Respiratory physiology and respiratory function during anesthesia. In: Miller RD (ed) Miller’s anesthesia. Churchill Livingstone, New York, p 697
Ochoa ME, Marin Mdel C, Frutos-Vivar F et al (2009) Cuff-leak test for the diagnosis of upper airway obstruction in adults: a systematic review and meta-analysis. Intensive Care Med 35:1171–1179
Miller RL, Cole RP (1996) Association between reduced cuff leak volume and postextubation stridor. Chest 110:1035–1040
Sandhu RS, Pasquale MD, Miller K et al (2000) Measurement of endotracheal tube cuff leak to predict postextubation stridor and need for reintubation. J Am Coll Surg 190:682–687
Lakhal K, Delplace X, Cottier JP et al (2007) The feasibility of ultrasound to assess subglottic diameter. Anesth Analg 104:611–614
Kristensen MS (2011) Ultrasonography in the management of the airway. Acta Anaesthesiol Scand 55:1155–1173
Ding LW, Wang HC, Wu HD et al (2006) Laryngeal ultrasound: a useful method in predicting post-extubation stridor. A pilot study. Eur Respir J 27:384–389
Antonucci S, Orlandi P, Mattei PA et al (2006) Airway obstruction during arthroscopic shoulder surgery: anesthesia for the patient or for the surgeon? Minerva Anestesiol 72:995–1000
Gal TJ (2005) Pulmonary function testing. In: Miller RD (ed) Miller’s anesthesia. Churchill Livingstone, New York, p 1001
Al-Kaisy AA, Chan VW, Perlas A (1999) Respiratory effects of low-dose bupivacaine interscalene block. Br J Anaesth 82:217–220
Bigliani LU, Flatow EL, Deliz ED (1991) Complications of shoulder arthroscopy. Orthop Rev 20:743–751
Borgeat A, Bird P, Ekatodramis G et al (2000) Tracheal compression caused by periarticular fluid accumulation: a rare complication of shoulder surgery. J Shoulder Elbow Surg 9:443–445
Matthews LS, Fadale PD (1989) Subacromial anatomy for the arthroscopist. Arthroscopy 5:36–40
Noyes FR, Spievack ES (1982) Extraarticular fluid dissection in tissues during arthroscopy. A report of clinical cases and a study of intraarticular and thigh pressures in cadavers. Am J Sports Med 10:346–351
Freedman B (1950) Unilateral paralysis of the diaphragm and larynx associated with inflammatory lung disease. Thorax 5:169–182
Conflict of interest
The corresponding author states that there are no conflicts of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Gwak, M., Kim, W., Choi, S. et al. Arthroscopic shoulder surgery under general anesthesia with brachial plexus block. Anaesthesist 62, 113–120 (2013). https://doi.org/10.1007/s00101-012-2125-y
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00101-012-2125-y
Keywords
- Respiratory function tests
- Airway obstruction
- Rotator cuff
- Complications
- Extravasation of diagnostic, therapeutic materials