
Abstract
Purpose
Surgical stabilization of rib fractures (SSRF) improves outcomes in certain patient populations. The Chest Wall Injury Society (CWIS) began a new initiative to recognize centers who epitomize their mission as CWIS Collaborative Centers (CWIS-CC). We sought to describe incidence and epidemiology of SSRF at our institutions.
Methods
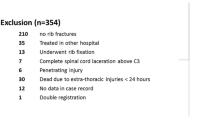
A retrospective registry evaluation of all patients (age > 15 years) treated at international trauma centers from 1/1/20 to 7/30/2021 was performed. Variables included: age, gender, mechanism of injury, injury severity score, abbreviated injury severity score (AIS), emergency department disposition, length of stay, presence of rib/sternal fractures, and surgical stabilization of rib/sternal fractures. Classification and regression tree analysis (CART) was used for analysis.
Results
Data were collected from 9 centers, 26,084 patient encounters. Rib fractures were present in 24% (n = 6294). Overall, 2% of all patients underwent SSRF and 8% of patients with rib fractures underwent SSRF. CART analysis of SSRF by AIS-Chest demonstrated a difference in management by age group. AIS-Chest 3 had an SSRF rate of 3.7, 7.3, and 12.9% based on the age ranges (16–19; 80–110), (20–49; 70–79), and (50–69), respectively (p = 0.003). AIS-Chest > 3 demonstrated an SSRF rate of 9.6, 23.3, and 39.3% for age ranges (16–39; 90–99), (40–49; 80–89), and (50–79), respectively (p = 0.001).
Conclusion
Anticipated rate of SSRF can be calculated based on number of rib fractures, AIS-Chest, and age. The disproportionate rate of SSRF in patients age 50–69 with AIS-Chest 3 and age 50–79 with AIS-Chest > 3 should be further investigated, as lower frequency of SSRF in the other age ranges may lead to care inequalities.


Similar content being viewed by others


Data availability
Data is not publically available.
References
Ziegler DW, Agarwal NN. The morbidity and mortality of rib fractures. J Trauma. 1994;37(6):975–9.
Choi J, et al. Prospective study of long-term quality-of-life after rib fractures. Surgery. 2022;172(1):404–9.
Choi J, et al. Prospective study of short-term quality-of-life after traumatic rib fractures. J Trauma Acute Care Surg. 2021;90(1):73–8.
Bemelman M, et al. Rib fractures: to fix or not to fix? An evidence-based algorithm. Korean J Thorac Cardiovasc Surg. 2017;50(4):229–34.
Senekjian L, et al. Stop flailing: the impact of bicortically displaced rib fractures on pulmonary outcomes in patients with chest trauma—an American Association for the Surgery of Trauma multi-institutional study. J Trauma Acute Care Surg. 2020;89(4):658–64.
Bulger EM, et al. Rib fractures in the elderly. J Trauma. 2000;48(6):1040–6 (discussion 1046–7).
Prins JTH, et al. Long-term pulmonary function, thoracic pain, and quality of life in patients with one or more rib fractures. J Trauma Acute Care Surg. 2021;91(6):923–31.
Witt CE, Bulger EM. Comprehensive approach to the management of the patient with multiple rib fractures: a review and introduction of a bundled rib fracture management protocol. Trauma Surg Acute Care Open. 2017;2(1): e000064.
Deloney LP, et al. Efficacy of methocarbamol for acute pain management in young adults with traumatic rib fractures. Ann Pharmacother. 2021;55(6):705–10.
Doben AR, et al. Surgical rib fixation for flail chest deformity improves liberation from mechanical ventilation. J Crit Care. 2014;29(1):139–43.
Pieracci FM, et al. A multicenter, prospective, controlled clinical trial of surgical stabilization of rib fractures in patients with severe, nonflail fracture patterns (Chest Wall Injury Society NONFLAIL). J Trauma Acute Care Surg. 2020;88(2):249–57.
Pieracci FM, et al. Surgical stabilization of rib fractures in octogenarians and beyond-what are the outcomes? J Trauma Acute Care Surg. 2021;90(6):1014–21.
Prins JTH, et al. Outcome after surgical stabilization of rib fractures versus nonoperative treatment in patients with multiple rib fractures and moderate to severe traumatic brain injury (CWIS-TBI). J Trauma Acute Care Surg. 2021;90(3):492–500.
Wijffels MME, et al. Operative versus nonoperative treatment of multiple simple rib fractures: a systematic review and meta-analysis. Injury. 2020;51(11):2368–78.
Wijffels MME, et al. Early fixation versus conservative therapy of multiple, simple rib fractures (FixCon): protocol for a multicenter randomized controlled trial. World J Emerg Surg. 2019;14:38.
Kourouche S, et al. Development of a blunt chest injury care bundle: an integrative review. Injury. 2018;49(6):1008–23.
Forrester JD, et al. Chest wall injury centers-how we did it. J Thorac Dis. 2021;13(10):6104–7.
Kane ED, et al. Quantifying and exploring the recent national increase in surgical stabilization of rib fractures. J Trauma Acute Care Surg. 2017;83(6):1047–52.
Ali-Osman F, et al. Geriatric (G60) trauma patients with severe rib fractures: is muscle sparing minimally invasive thoracotomy rib fixation safe and does it improve post-operative pulmonary function? Am J Surg. 2018;216(1):46–51.
Tignanelli CJ, et al. Association between adherence to evidence-based practices for treatment of patients with traumatic rib fractures and mortality rates among US trauma centers. JAMA Netw Open. 2020;3(3): e201316.
Skinner M, et al. Rib season: temporal variation in chest wall injuries. J Surg Res. 2021;260:129–33.
Author information
Authors and Affiliations
Contributions
EAE, ARD, and JDF participated in the literature search. EAE, MMEW, AK, ARD, JDF, SM, ZMB, CFJ, BP, and MW participated in the study design. EAE, MMEW, AK, ARD, JDF, SM, ZMB, CFJ, BP, MW, MM, LC, SC, EMMVL, JT, MW, RH, and TW participated in data collection. EAE performed the data analysis. EAE, MMEW, AK, ARD, JDF, SM, ZMB, CFJ, BP, and MW participated in data interpretation. EAE and ARD drafted the article. EAE, MMEW, AK, ARD, JDF, SM, ZMB, CFJ, BP, MW, MM, LC, SC, EMMVL, JT, MW, RH, and TW participated in critical revisions. All authors approved the final article version for submission.
Corresponding author
Ethics declarations
Conflict of interest
EAE—Speaker for DePuy Synthes. Dr. Forrester has received unrestricted research funding from Varian for an investigator-initiated clinical trial (https://clinicaltrials.gov/ct2/show/NCT04482582) and received grant funding from the Surgical Infections Society. Neither of these lead to conflicts of interest for this work product. JT: No disclosures. MEW: No disclosures. MMEW—Ad hoc advisor for Johnson & Johnson DePuy Synthes, Research funding Johnson & Johnson DePuySynthes, Research funding Osteosynthesis and Trauma Foundation (OTC). MEW(Wullschleger): Ad hoc advisor for Johnson & Johnson DePuySynthes. AK (Kaye): Lecturer Zimmer/Biomet, and Atricure. AD: Past consultant for DePuy Synthes, KLS-Martin, Zimmer-Biomet. No current relationships related to this project. BP: no disclosures. EMMVL—No disclosures. ZMB: Paid educational consultant for Zimmer-Biomet, KLS-Martin, and Atricure. LC no disclosures. SC no disclosures. SM—none. CJ—none. TRH—none. MM—none.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Eriksson, E.A., Wijffels, M.M.E., Kaye, A. et al. Incidence of surgical rib fixation at chest wall injury society collaborative centers and a guide for expected number of cases (CWIS-CC1). Eur J Trauma Emerg Surg 50, 417–423 (2024). https://doi.org/10.1007/s00068-023-02343-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00068-023-02343-4