
Abstract
Background
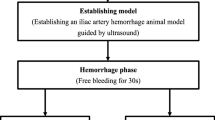
Endovascular balloon occlusion of the aorta (EBOA) increases proximal arterial pressure but may also induce life-threatening ischemic complications. Although partial REBOA (P-REBOA) mitigates distal ischemia, it requires invasive monitoring of femoral artery pressure for titration. In this study, we aimed to titrate P-REBOA to prevent high-degree P-REBOA using ultrasound assessment of femoral arterial flow.
Methods
Proximal (carotid) and distal (femoral) arterial pressures were recorded, and perfusion velocity of distal arterial pressures was measured by pulse wave Doppler. Systolic and diastolic peak velocities were measured among all ten pigs. Total REBOA was defined as a cessation of distal pulse pressure, and maximum balloon volume was documented. The balloon volume (BV) was titrated at 20% increments of maximum capacity to adjust the degree of P-REBOA. The distal/proximal arterial pressure gradient and the perfusion velocity of distal arterial pressures were recorded.
Results
Proximal blood pressure increased with increasing BV. Distal pressure decreased with increasing BV, and distal pressure sharply decreased by > 80% of BV. Both systolic and diastolic velocities of the distal arterial pressure decreased with increasing BV. Diastolic velocity could not be recorded when the BV of REBOA was > 80%.
Conclusion
The diastolic peak velocity in the femoral artery disappeared when %BV was > 80%. Evaluation of the femoral artery pressure by pulse wave Doppler may predict the degree of P-REBOA without invasive arterial monitoring.






Similar content being viewed by others

Data availability
The data that support the findings of this study are available from the corresponding author, YM, upon reasonable request.
References
Brenner M, Inaba K, Aiolfi A, AAST AORTA Study Group, et al. Resuscitative endovascular balloon occlusion of the aorta and resuscitative thoracotomy in select patients with hemorrhagic shock: early results from the American Association for the surgery of Trauma’s aortic occlusion in resuscitation for trauma and acute care surgery registry. J Am Coll Surg. 2018;226(5):730–40.
Johnson NL, Wade CE, Fox EE, Emergent Truncal Hemorrhage Control Study Group, et al. Determination of optimal deployment strategy for REBOA in patients with non-compressible hemorrhage below the diaphragm. Trauma Surg Acute Care Open. 2021;6(1):e000660.
Laverty RB, Treffalls RN, McEntire SE, Aortic Occlusion for Resuscitation in Trauma and Acute Care Surgery (AORTA) Investigators, et al. Life over limb: arterial access-related limb ischemic complications in 48-hour REBOA survivors. J Trauma Acute Care Surg. 2022;92(4):723–8.
Joseph B, Zeeshan M, Sakran JV, et al. Nationwide analysis of resuscitative endovascular balloon occlusion of the aorta in civilian trauma. JAMA Surg. 2019;154(6):500–8.
Manzano-Nunez R, Orlas CP, Herrera-Escobar JP, et al. A meta-analysis of the incidence of complications associated with groin access after the use of resuscitative endovascular balloon occlusion of the aorta in trauma patients. J Trauma Acute Care Surg. 2018;85(3):626–34.
Russo RM, White JM, Baer DG. Partial resuscitative endovascular balloon occlusion of the aorta: a systematic review of the preclinical and clinical literature. J Surg Res. 2021;262:101–14.
Kemp MT, Wakam GK, Williams AM, et al. A novel partial resuscitative endovascular balloon aortic occlusion device that can be deployed in zone 1 for more than 2 hours with minimal provider titration. J Trauma Acute Care Surg. 2021;90(3):426–33.
Forte DM, Do WS, Weiss JB, et al. Validation of a novel partial resuscitative endovascular balloon occlusion of the aorta device in a swine hemorrhagic shock model: fine tuning flow to optimize bleeding control and reperfusion injury. J Trauma Acute Care Surg. 2020;89(1):58–67.
Russo RM, Neff LP, Lamb CM, et al. Partial resuscitative endovascular balloon occlusion of the aorta in swine model of hemorrhagic shock. J Am Coll Surg. 2016;223(2):359–68.
Matsumura Y, Higashi A, Izawa Y, et al. Distal pressure monitoring and titration with percent balloon volume: feasible management of partial resuscitative endovascular balloon occlusion of the aorta (P-REBOA). Eur J Trauma Emerg Surg. 2021;47(4):1023–9.
Matsumura Y, Higashi A, Izawa Y, et al. Organ ischemia during partial resuscitative endovascular balloon occlusion of the aorta: dynamic 4D computed tomography in swine. Sci Rep. 2020;10(1):5680.
Teeter WA, Matsumoto J, Idoguchi K, et al. Smaller introducer sheaths for REBOA may be associated with fewer complications. J Trauma Acute Care Surg. 2016;81(6):1039–45.
Inoue J, Shiraishi A, Yoshiyuki A, et al. Resuscitative endovascular balloon occlusion of the aorta might be dangerous in patients with severe torso trauma: a propensity score analysis. J Trauma Acute Care Surg. 2016;80(4):559–66 (discussion 566–7).
Plurad DS, Chiu W, Raja AS, et al. Monitoring modalities and assessment of fluid status: a practice management guideline from the Eastern Association for the Surgery of Trauma. J Trauma Acute Care Surg. 2018;84(1):37–49.
Dinsmore M, Venkatraghavan L. Clinical applications of point-of-care ultrasound in brain injury: a narrative review. Anaesthesia. 2022;77(Suppl 1):69–77.
Reva VA, Perevedentcev AV, Pochtarnik AA, et al. Ultrasound-guided versus blind vascular access followed by REBOA on board of a medical helicopter in a hemorrhagic ovine model. Injury. 2021;52(2):175–81.
Qadri HI, Patel NT, Ganapathy AS, et al. Maintaining zone 1 occlusion is a dynamic process: the effects of proximal pressure and blood transfusion during REBOA. Am Surg. 2022;88(7):1496–503.
Funding
This study was supported in part by ZENKYOREN (National Mutual Insurance Federation of Agricultural Cooperatives), 2021–2022.
Author information
Authors and Affiliations
Contributions
Corresponding author YM. Study concept, design MA, YM, YI. Data collection and analysis: MA, YM, YI, YH. Writing: MA, YM. Critical revision: YM, YI, YH.
Corresponding author
Ethics declarations
Conflict of interest
No conflicts are declared.
Ethical approval and consent to participate
All procedures were approved by the Centre for Development of Advanced Medical Technology from Jichi Medical University.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Aoki, M., Matsumura, Y., Izawa, Y. et al. Ultrasound assessment is useful for evaluating balloon volume of resuscitative endovascular balloon occlusion of the aorta. Eur J Trauma Emerg Surg 49, 2479–2484 (2023). https://doi.org/10.1007/s00068-023-02309-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00068-023-02309-6