
Abstract
Background
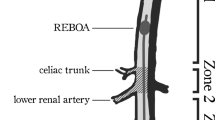
Resuscitative endovascular balloon occlusion of the aorta (REBOA) can timely prevent the wounded from fatal hemorrhage. However, blind insertion of REBOA in field or emergency room may result in catheter malposition and serious complications. We aim to develop a new method based on surface landmarks to guide the accurate placement of REBOA in zone III of aorta without fluoroscopy.
Methods
A retrospective study was conducted in a university hospital, including 57 subjects who underwent computed tomography angiography (CTA) from April to December in 2019. External distances and intravascular lengths were measured by three-dimensional reconstruction of CT images, including the distances from the insertion site of femoral artery to the xiphoid process (FA-Xi), the midpoint between the xiphoid process and the umbilicus (FA-mXU), the umbilicus (FA-Ui), the midpoint of the zone III of aorta (FA-mZIII), the lowest renal artery (FA-LRA), and aortic bifurcation (FA-AB). The distal and proximal ideal margin and predicted accuracy were calculated by curvature plane reconstruction. The predicted probability of balloon positioning in zone III by different methods was compared.
Results
The mean age of all patients was 60 years (SD = 9.4). The average length of zone III of aorta was 9.4 cm (SD = 1.0), and the length of FA-mZIII on the right and left sides were 24.4 cm (SD = 2.1), 23.8 cm (SD = 2.1), respectively. FA-Xi was longer than FA-LRA, and FA-Ui was shorter than FA-AB (paired two-tailed test, p < 0.001). Using three methods including the optimal quartering distances, the optimal distances below the xiphoid and above the umbilicus to predict the length of REBOA catheter positioning in zone III showed no statistically significant difference. The predicted accuracy of catheter positioning in zone III on the left and right sides guided by FA-mXU were 84.2% and 86%.
Conclusions
The midpoint between the xiphoid process and the umbilicus may be a new surface landmark for people of normal weight to guide rapid positioning REBOA in zone III of aorta without fluoroscopy.





Similar content being viewed by others


Availability of data and material
All the data are available and will be submitted if required.
Code availability
Software application.
Abbreviations
- REBOA:
-
Resuscitative endovascular balloon occlusion of the aorta
- CTA:
-
Computed tomography angiography
- FA:
-
Femoral artery
- Xi:
-
Xiphoid process
- mXU:
-
The midpoint between the xiphoid process and the umbilicus
- Ui:
-
Umbilicus
- mZIII:
-
The midpoint of the zone III
- BMI:
-
Body mass index
- LRA:
-
Lowest renal artery
- AB:
-
Aortic bifurcation
References
Joyce MF, Gupta A, Azocar RJ. Acute trauma and multiple injuries in the elderly population. Curr Opin Anaesthesiol. 2015;28(2):145–50.
GBD 2016 Causes of Death Collaborators. Global, regional, and national age-sex specific mortality for 264 causes of death, 1980–2016: a systematic analysis for the global burden of disease study 2016. Lancet. 2017;390(10100):1151–210.
Prionas A, Tsoulfas G, Tooulias A, et al. Evaluating trauma care, outcomes and costs in a system in crisis: the necessity of a Greek national trauma database. Trauma Surg Acute Care Open. 2020;5(1):e00040.
Atinga A, Shekkeris A, Fertleman M, et al. Trauma in the elderly patient. Br J Radiol. 2018;91(1087):20170739.
Cannon JW, Khan MA, Raja AS, Cohen MJ, Como JJ, Cotton BA, et al. Damage control resuscitation in patients with severe traumatic hemorrhage: a practice management guideline from the eastern association for the surgery of trauma. J Trauma Acute Care Surg. 2017;82(3):605–17.
Fox EE, Holcomb JB, Wade CE, Bulger EM, Tilley BC. Earlier endpoints are required for hemorrhagic shock trials among severely injured patients. Shock. 2017;47(5):567–73.
Henry R, Matsushima K, Henry RN, Wong V, Warriner Z, Strumwasser A, et al. Who would have benefited from the prehospital use of resuscitative endovascular balloon occlusion of the aorta (REBOA)? An autopsy study. J Am Coll Surg. 2019;229(4):383–8 (e1).
Eliason JL, Derstine BA, Horbal SR, Wang NC, Holcombe SA, Chiu CH, et al. Computed tomography correlation of skeletal landmarks and vascular anatomy in civilian adult trauma patients: implications for resuscitative endovascular balloon occlusion of the aorta. J Trauma Acute Care Surg. 2019;87(1S Suppl 1):S138–45.
Pezy P, Flaris AN, Prat NJ, Cotton F, Lundberg PW, Caillot J-L, et al. Fixed-distance model for balloon placement during fluoroscopy-free resuscitative endovascular balloon occlusion of the aorta in a civilian population. JAMA Surg. 2017;152(4):351–8.
Meyer DE, Mont MT, Harvin JA, Kao LS, Wade CE, Moore LJ. Catheter distances and balloon inflation volumes for the ER-REBOATM catheter: a prospective analysis. Am J Surg. 2020;219(1):140–4.
Linnebur M, Inaba K, Haltmeier T, Rasmussen TE, Smith J, Mendelsberg R, et al. Emergent non-image-guided resuscitative endovascular balloon occlusion of the aorta (REBOA) catheter placement: a cadaver-based study. J Trauma Acute Care Surg. 2016;81(3):453–7.
Okada Y, Narumiya H, Ishi W, Iiduka R. Anatomical landmarks for safely implementing resuscitative balloon occlusion of the aorta (REBOA) in zone 1 without fluoroscopy. Scand J Trauma Resusc Emerg Med. 2017;25(1):63.
Liu X, He Y, Zhu Q, Gao F, He W, Yu L, et al. Supra-annular structure assessment for self-expanding transcatheter heart valve size selection in patients with bicuspid aortic valve. Catheter Cardiovasc Interv. 2018;91(5):986–94.
Stannard A, Eliason JL, Rasmussen TE. Resuscitative endovascular balloon occlu- sion of the aorta (REBOA) as an adjunct for hemorrhagic shock. J Trauma. 2011;71(6):1869–72.
Bulger EM, Perina DG, Qasim Z, Beldowicz B, Brenner M, Guyette F, Stewart R, et al. Clinical use of resuscitative endovascular balloon occlusion of the aorta (REBOA) in civilian trauma systems in the USA, 2019: a joint statement from the American College of Surgeons Committee on Trauma, the American College of Emergency Physicians, the National Association of Emergency Medical Services Physicians and the National Association of Emergency Medical Technicians. Trauma Surg Acute Care Open. 2019;4(1):e000376.
Wessels LE, Wallace JD, Bowie J, Butler WJ, Spalding C, Krzyzaniak M. Radiofrequency identification of the ER-REBOA: confirmation of placement without fluoroscopy. Mil Med. 2019;184(3–4):e285–9.
MacTaggart JN, Poulson WE, Akhter M, Seas A, Thorson K, Phillips NY, et al. Morphometric roadmaps to improve accurate device delivery for fluoroscopy-free resuscitative endovascular balloon occlusion of the aorta. J Trauma Acute Care Surg. 2016;80(6):941–6.
Park Y, Jo YG, Choi K-H, Kim M, Kim J. Gamma probe-guided confirmation of balloon placement in endovascular procedures. J Trauma Acute Care Surg. 2019;86(6):994–1000.
Rezende-Neto JB, Ravi A, Semple M. Magnetically trackable resuscitative endovascular balloon occlusion of the aorta: a new non-image-guided technique for resuscitative endovascular balloon occlusion of the aorta. J Trauma Acute Care Surg. 2020;88(2):e87–91.
Martinelli T, Thony F, Decléty P, Sengel C, Broux C, Tonetti J, et al. Intra-aortic balloon occlusion to salvage patients with life-threatening hemorrhagic shocks from pelvic fractures. J Trauma. 2010;68(4):942–8.
Funding
Mao Zhang is funded by the Key Program Co-sponsored by Zhejiang Province and National Health Commission of China (2018271879) and the Key Research Project of Zhejiang Province (2021C03073). Anyu Qian is funded by the Welfare Scientific Research Project of Zhejiang Province (LGD19H150003). These agencies provided financial support but were not involved in any other aspect of the research.
Author information
Authors and Affiliations
Contributions
The corresponding author (MZ and SX) was in charge of study design and data analysis. The first author (DW) was responsible for data collection, manuscript writing and cooperated with the rest three authors (AQ, QZ, and JX) in data analysis and correction work. All authors participated in the critical revision of the manuscript, and all authors approved the final version to be submitted.
Corresponding authors
Ethics declarations
Conflict of interest
The authors declare that they have no competing interests.
Ethics approval and consent to participate
This retrospective study was approved by the Ethics Committee of the Second Affiliated Hospital of Zhejiang University School of Medicine (approval number: 2019380).
Rights and permissions
About this article

Cite this article
Weng, D., Qian, A., Zhou, Q. et al. A new method using surface landmarks to locate resuscitative endovascular balloon occlusion of the aorta based on a retrospective CTA study. Eur J Trauma Emerg Surg 48, 1945–1953 (2022). https://doi.org/10.1007/s00068-021-01686-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00068-021-01686-0