
Abstract
Objective
To study the relationship between the pelvic external branches of the superior gluteal artery and the entry area of the S2 sacroiliac screw to provide the anatomical basis and technical reference for avoiding the superior gluteal artery injury during the clinical screw placement.
Methods
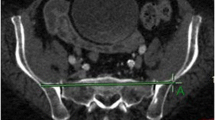
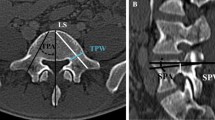
CTA imaging of superior gluteal artery of 74 healthy adults (37 males and 37 females) was randomly selected. The safe bony entry area (‘safe area’ for abbreviation) of S2 sacroiliac screw in the standard lateral view of the pelvis three-dimensional reconstruction CT image was determined by the CT auxiliary measurement software. The relationship between the pelvic external branches of the superior gluteal artery and the safe area of S2 sacroiliac screw was observed, and the cases in which the artery intersected the safe area were counted. The distance between the safe area and the superior gluteal artery branches closest to it was measured for the cases in which the artery and the safe area did not intersect.
Results
21 of the 74 cases did not have a bone channel of horizontal S2 sacroiliac screw, so they were excluded from this study. In the remaining 53 cases, 12 cases had the deep superior branch of the superior gluteal artery through the safe area of S2 screw (22.6%), and 16 cases had the superficial branch of the superior gluteal artery through the safe area of S2 screw (30.2%). There was no obvious overlap feature and law between the safe area and the superficial and deep superior branches. In 20 cases of the 53 cases, the safe area of S2 screw was located between the deep superior branch and the superficial branch of superior gluteal artery (37.7%), and in 5 cases, the safe area of S2 screw was located behind the superficial branch of superior gluteal artery (9.4%). In the cases where the superior gluteal artery did not intersect the screw entry bony safe area, the part of superior gluteal artery closest to the safe area was located in front or back of the widest part of the safe area.
Conclusion
The risk of accidental injury of the deep superior branch and superficial branch of the superior gluteal artery is high during the process of S2 sacroiliac screw placement. Even if the screw entry point is located in the bony safe area, the absolute safety of screw placement cannot be guaranteed. We strongly suggest that a careful and thorough plan is needed before surgery.


Similar content being viewed by others

References
Dujardin FH, Roussignol X, Hossenbaccus M, Thomine JM. Experimental study of the sacroiliac joint micromotion in pelvic disruption. J Orthop Trauma. 2002;16:99–103.
Tucker MC, Nork SE, Simonian PT, Routt ML Jr. Simple anterior pelvic external fixation. J Trauma. 2000;49:989–94.
Vallier HA, Cureton BA, Ekstein C, Oldenburg FP, Wilber JH. Early definitive stabilization of unstable pelvis and acetabulum fractures reduces morbidity. J Trauma. 2010;69:677–84.
Enninghorst N, Toth L, King KL, McDougall D, Mackenzie S, Balogh ZJ. Acute definitive internal fixation of pelvic ring fractures in polytrauma patients: a feasible option. J Trauma. 2010;68:935–41.
Shuler TE, Boone DC, Gruen GS, Peitzman AB. Percutaneous iliosacral screw fixation: early treatment for unstable posterior pelvic ring disruptions. J Trauma. 1995;38:453–8.
Marmor M, Lynch T, Matityahu A. Superior gluteal artery injury during iliosacral screw placement due to aberrant anatomy. Orthopedics. 2010;33:117–20.
Maled I, Velez R, Lopez R, Batalla L, Caja VL. Pseudoaneurysm of the superior gluteal artery during iliosacral screw fixation. Acta Orthop Belg. 2007;73:544–7.
Altman DT, Jones CB, Routt ML Jr. Superior gluteal artery injury during iliosacral screw placement. J Orthop Trauma. 1999;13:220–7.
Stephen DJG. Pseudoaneurysm of the superior gluteal arterial system: an unusual cause of pain after pelvic fracture. J Trauma. 1997;43:146–9.
Carlson DA, Scheid DK, Maar DC, Baele JR, Kaehr DM. Safe placement of S1 and S2 iliosacral screws: the “vestibule” concept. J Orthop Trauma. 2000;14:264–9.
Day CS, Prayson MJ, Shuler TE, Towers J, Gruen GS. Transsacral versus modified pelvic and marks for percutaneous iliosacral screw placement—a computed tomographic analysis and cadaveric study. Am J Orthop. 2000;29(9 suppl):16–21.
Zhao Y, Li J, Wang D, Lian W. Parameters of lengthened sacroiliac screw fixation: a radiological anatomy study. Eur Spine J. 2012;21:1807–14.
Zhao Y, Li J, Wang D, Liu Y, Tan J, Zhang S. Comparison of stability of two kinds of sacro-iliac screws in the fixation of bilateral sacral fractures in a finite element model. Injury. 2012;43:490–4.
Zhao Y, Zhang S, Sun T, Wang D, Lian W, Tan J, Zou D, Zhao Y. Mechanical comparison between lengthened and short sacroiliac screws in sacral fracture fixation: a finite element analysis. Orthop Traumatol Surg Res. 2013;99:601–6.
Fu S, Zhao Y, Lian W, Zou D, Sun T, Zhao Y, Tan J, Zhang S, Wang D. Comparison of the risk of breakage of two kinds of sacroiliac screws in the treatment of bilateral sacral fractures. Eur Spine J. 2014;23:1558–67.
Collinge C, Coons D, Aschenbrenner J. Risks to the superior gluteal neurovascular bundle during percutaneous iliosacral screw insertion: an anatomical cadaver study. J Orthop Trauma. 2005;19:96–101.
Conflitti JM, Graves ML, Chip Routt ML. Radiographic quantification and analysis of dysmorphic upper sacral osseous anatomy and associated iliosacral screw insertions. J Orthop Trauma. 2010;24:630–6.
Gardner MJ, Morshed S, Nork SE, Ricci WM, Chip Routt ML Jr. Quantification of the upper and second sacral segment safe zones in normal and dysmorphic sacra. J Orthop Trauma. 2010;24:622–9.
Yinger K, Scalise J, Olson SA, Bay BK, Finkemeier CG. Biomechanical comparison of posterior pelvic ring fixation. J Orthop Trauma. 2003;17:481–7.
van Zwienen CM, van den Bosch EW, Snijders CJ, Kleinrensink GJ, van Vugt AB. Biomechanical comparison of sacroiliac screw techniques for unstable pelvic ring fractures. J Orthop Trauma. 2004;18:589–95.
Funding
This research was supported by the National Natural Science Foundation of China (no. 81301553 and no. 81641171), Distinguished Middle-Aged and Young Scientist Encourage and Reward Foundation of Shandong Province, China (no. BS2013SF015), Shandong Provincial Key R&D Program of China (no. 2018GSF118064), Project of Medical and Health Technology Development Program of Shandong Province, China (no. 2017WS169), Project of Traditional Chinese Medicine Science and Technology Development Program of Shandong Province, China (no. 2017-391) and Project of Science and Technology Development Program of Yantai City, China (no. 2010149-10, no. 2013WS234, and no. 2016WS036).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Yong Zhao, Wenliang Li, Wei Lian, Jingning Li, Dexin Zou, Xiujiang Sun, Gong Cheng, Shengjie Dong and Tao Sun declare that they have no conflict of interest.
Ethical approval
The study was approved by the ethics committees of Yantai Shan Hospital.
Informed consent
Informed consent was obtained from all individual participants included in this study.
Rights and permissions
About this article

Cite this article
Zhao, Y., Li, W., Lian, W. et al. Anatomic relationship between S2 sacroiliac screws’ entry points and pelvic external branches of superior gluteal artery. Eur J Trauma Emerg Surg 48, 857–862 (2022). https://doi.org/10.1007/s00068-021-01622-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00068-021-01622-2