
Abstract
Purpose
In patients with traumatic pelvic fractures, thromboelastography (TEG) is a useful tool to rapidly evaluate and identify coagulation disturbances. The purpose of this study was to examine the coagulation kinetics of patients with traumatic pelvic fractures (pelvic ring and/or acetabulum) by analyzing the TEG results at initial presentation and its relationship with mortality and blood loss.
Methods
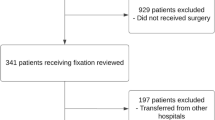
A retrospective review at our Level-1 trauma center was conducted to identify Full Trauma Team activations (FTTa) with traumatic pelvic and/or acetabular fractures who were evaluated with a TEG on initial presentation between 2012 and 2016. In-hospital mortality, product transfusion, and hemoglobin changes were analyzed. Subgroup analysis was performed based on pelvic fracture type.
Results
141 patients with a mean age of 49.0 ± 20.8 years and mean Injury Severity Score (ISS) of 25.18 ± 12.8 met inclusion criteria. PRBC transfusion occurred in 78.0% of patients; a total of 1486 blood products were transfused. A total of 65 patients (46.1%) underwent operative treatment for the pelvic injuries, and 18 patients (12.7%) required embolization. The overall in-hospital mortality rate was 14.9%. The degree of clot lysis at 30 min (LY30) was significantly associated with blood loss (p < 0.0001), units of packed red blood cells (PRBCs) transfused (p < 0.0001), and mortality rate (p = 0.0002).
Conclusion
Increased fibrinolysis evidenced by an elevated LY30 on initial TEG in patients with traumatic pelvic fractures is associated with increased blood loss, blood product transfusions, and mortality. Future studies should evaluate the clinical utility of reversing hyperfibrinolysis on initial TEG.
Level of evidence
Prognostic level III.
Similar content being viewed by others


Data availability
Reasonable requests will be considered.
References
Langford JR, Burgess AR, Liporace FA, Haidukewych GJ. Pelvic fractures: part 1. Evaluation, classification, and resuscitation. J Am Acad Orthop Surg. 2013;21(8):448–57.
Giannoudis PV, Pape HC. Damage control orthopaedics in unstable pelvic ring injuries. Injury. 2004;35(7):671–7.
Starr AJ, Griffin DR, Reinert CM, Frawley WH, Walker J, Whitlock SN, et al. Pelvic ring disruptions: prediction of associated injuries, transfusion requirement, pelvic arteriography, complications, and mortality. J Orthop Trauma. 2002;16(8):553–61.
Osborn PM, Smith WR, Moore EE, Cothren CC, Morgan SJ, Williams AE, et al. Direct retroperitoneal pelvic packing versus pelvic angiography: a comparison of two management protocols for haemodynamically unstable pelvic fractures. Injury. 2009;40(1):54–60.
Demetriades D, Karaiskakis M, Toutouzas K, Alo K, Velmahos G, Chan L. Pelvic fractures: epidemiology and predictors of associated abdominal injuries and outcomes. J Am Coll Surg. 2002;195(1):1–10.
Rossaint R, Cerny V, Coats TJ, Duranteau J, Fernandez-Mondejar E, Gordini G, et al. Key issues in advanced bleeding care in trauma. Shock. 2006;26(4):322–31.
Agolini SF, Shah K, Jaffe J, Newcomb J, Rhodes M, Reed JF 3rd. Arterial embolization is a rapid and effective technique for controlling pelvic fracture hemorrhage. J Trauma. 1997;43(3):395–9.
Velmahos GC, Toutouzas KG, Vassiliu P, Sarkisyan G, Chan LS, Hanks SH, et al. A prospective study on the safety and efficacy of angiographic embolization for pelvic and visceral injuries. J Trauma. 2002;53(2):303–8 (Discussion 8).
Spahn DR, Cerny V, Coats TJ, Duranteau J, Fernandez-Mondejar E, Gordini G, et al. Management of bleeding following major trauma: a European guideline. Crit Care. 2007;11(1):R17.
Huittinen VM, Slatis P. Postmortem angiography and dissection of the hypogastric artery in pelvic fractures. Surgery. 1973;73(3):454–62.
Platz A, Friedl HP, Kohler A, Trentz O. Surgical management of severe pelvic crush injuries. Helv Chir Acta. 1992;58(6):925–9.
Da Luz LT, Nascimento B, Shankarakutty AK, Rizoli S, Adhikari NK. Effect of thromboelastography (TEG(R)) and rotational thromboelastometry (ROTEM(R)) on diagnosis of coagulopathy, transfusion guidance and mortality in trauma: descriptive systematic review. Crit Care. 2014;18(5):518.
Hagedorn JC 2nd, Bardes JM, Paris CL, Lindsey RW. Thromboelastography for the orthopaedic surgeon. J Am Acad Orthop Surg. 2019;27(14):503–8.
Roberts I, Shakur H, Ker K, Coats T. Antifibrinolytic drugs for acute traumatic injury. Cochrane Database Syst Rev. 2012;12:Cd004896.
Shakur H, Roberts I, Bautista R, Caballero J, Coats T, Dewan Y, et al. Effects of tranexamic acid on death, vascular occlusive events, and blood transfusion in trauma patients with significant haemorrhage (CRASH-2): a randomised, placebo-controlled trial. Lancet. 2010;376(9734):23–32.
Gonzalez E, Moore EE, Moore HB, Chapman MP, Chin TL, Ghasabyan A, et al. Goal-directed hemostatic resuscitation of trauma-induced coagulopathy: a pragmatic randomized clinical trial comparing a viscoelastic assay to conventional coagulation assays. Ann Surg. 2016;263(6):1051–9.
Schöchl H, Maegele M, Solomon C, Görlinger K, Voelckel W. Early and individualized goal-directed therapy for trauma-induced coagulopathy. Scand J Trauma Resusc Emerg Med. 2012;20:15.
Johansson PI, Stissing T, Bochsen L, Ostrowski SR. Thrombelastography and tromboelastometry in assessing coagulopathy in trauma. Scand J Trauma Resusc Emerg Med. 2009;17:45.
Morrison JJ, Dubose JJ, Rasmussen TE, Midwinter MJ. Military application of tranexamic acid in trauma emergency resuscitation (MATTERs) study. Arch Surg. 2012;147(2):113–9.
Mamczak CN, Maloney M, Fritz B, Boyer B, Thomas S, Evans E, et al. Thromboelastography in orthopaedic trauma acute pelvic fracture resuscitation: a descriptive pilot study. J Orthop Trauma. 2016;30(6):299–305.
Brohi K, Cohen MJ, Ganter MT, Schultz MJ, Levi M, Mackersie RC, et al. Acute coagulopathy of trauma: hypoperfusion induces systemic anticoagulation and hyperfibrinolysis. J Trauma. 2008;64(5):1211–7 (Discussion 7).
Holcomb JB, Minei KM, Scerbo ML, Radwan ZA, Wade CE, Kozar RA, et al. Admission rapid thrombelastography can replace conventional coagulation tests in the emergency department: experience with 1974 consecutive trauma patients. Ann Surg. 2012;256(3):476–86.
Cardenas JC, Rahbar E, Pommerening MJ, Baer LA, Matijevic N, Cotton BA, et al. Measuring thrombin generation as a tool for predicting hemostatic potential and transfusion requirements following trauma. J Trauma Acute Care Surg. 2014;77(6):839–45.
Brohi K, Singh J, Heron M, Coats T. Acute traumatic coagulopathy. J Trauma. 2003;54(6):1127–30.
Niles SE, McLaughlin DF, Perkins JG, Wade CE, Li Y, Spinella PC, et al. Increased mortality associated with the early coagulopathy of trauma in combat casualties. J Trauma. 2008;64(6):1459–63 (Discussion 63-5).
Davenport RA, Guerreiro M, Frith D, Rourke C, Platton S, Cohen M, et al. Activated protein C drives the hyperfibrinolysis of acute traumatic coagulopathy. Anesthesiology. 2017;126(1):115–27.
Hartert H. Not available. Klin Wochenschr. 1948;26(37–38):577–83.
Lance MD. A general review of major global coagulation assays: thrombelastography, thrombin generation test and clot waveform analysis. Thromb J. 2015;13:1.
Chapman MP, Moore EE, Ramos CR, Ghasabyan A, Harr JN, Chin TL, et al. Fibrinolysis greater than 3% is the critical value for initiation of antifibrinolytic therapy. J Trauma Acute Care Surg. 2013;75(6):961–7.
Acknowledgements
The authors would like to acknowledge the contribution of Tyler E. Calkins, MD, to data collection and processing for this study.
Funding
No funding was received in support of this work.
Author information
Authors and Affiliations
Contributions
PAB: Participated in study design, data collection, data analysis, and final manuscript preparation; JJR: Participated in study design, data collection, data analysis, and final manuscript preparation; BAK: Participated in study design, data collection, data analysis, and final manuscript preparation; MAB: Participated in study design, data analysis, and final manuscript preparation; AW: Participated in study design, and final manuscript preparation; MJD: Participated in study design, data collection, data analysis, and final manuscript preparation.
Corresponding author
Ethics declarations
Conflict of interest
The authors report no conflicts of interest or competing interests.
Ethical approval
Institutional Review Board approval was granted for this retrospective review.
Consent to participate
Not applicable.
Consent for publication
Not applicable.
Rights and permissions
About this article

Cite this article
Bostian, P.A., Ray, J.J., Karolcik, B.A. et al. Thromboelastography is predictive of mortality, blood transfusions, and blood loss in patients with traumatic pelvic fractures: a retrospective cohort study. Eur J Trauma Emerg Surg 48, 345–350 (2022). https://doi.org/10.1007/s00068-020-01533-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00068-020-01533-8