
Abstract
Introduction
Tranexamic acid (TXA) is one of the debated therapies in the management of traumatic brain injury (TBI). We conducted this study to evaluate the benefits of TXA in TBI on the mortality and its safety in these patients.
Methods
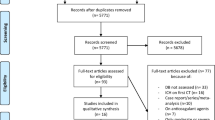
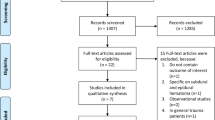
This was a prospective randomized open-label trial including all patients, aged at 18 years or older, hospitalized in the emergency room during a 13-month period, for TBI. After the realization of the body CT scan, the patients were included if they had intracranial bleeding, and were then randomized according to their medical file number to receive or not the TXA. The eligibility criteria were based on the uncertainty principle, patients with significant extracranial bleeding were excluded since there was evidence that TXA improve their outcome.
Results
We enrolled 180 patients aged at 42 ± 20 years, with an 88% men-proportion. Subarachnoid haemorrhage was the most frequent lesion in the brain CT-scan (67.5%). After randomization, 96 patients were in the TXA group (53%). Demographic data, clinical, biological and radiological features were statistically comparable in the two groups of patients (‘TXA’ and ‘noTXA’). The needs of transfusion or neurosurgery, the mortality rate, the in-hospital length of stay and the dependency at 28-post-traumatic day were similar in the two groups of patients. However, pulmonary embolism was statistically more frequent in ‘TXA’ group (11.5 versus 2.4%, p = 0.02).
Conclusion
TXA is an interesting treatment in haemorrhagic shock. Its efficiency in head trauma is still debated and controversial. Its impact on the mortality and the needs of transfusion or surgery were not demonstrated in this study. Nevertheless, its safety worth to be studied in larger samples as we found a higher rate of pulmonary embolism in the treated group.



Similar content being viewed by others

References
Chelly H, Bahloul M, Ammar R, et al. Clinical characteristics and prognosis of traumatic head injury following road traffic accidents admitted in ICU “analysis of 694 cases”. Eur J Trauma Emerg Surg. 2017. https://doi.org/10.1007/s00068-017-0885-4 (Epub ahead of print).
Bahloul M, Chelly H, Ben Hmida M, et al. Prognosis of traumatic head injury in South Tunisia: a multivariate analysis of 437 cases. J Trauma. 2004;57:255–61.
Jackisch J, Sethi D, Mitis F, et al. European facts and the Global status report on road safety. 2015; (WHO 2015). http://www.euro.who.int/__data/assets/pdf_file/0006/293082/European-facts-Global-Status-Report-road-safety-en.pdf. Accessed 15 June 2018.
Peeters W, van den Brande R, Polinder S, et al. Epidemiology of traumatic brain injury in Europe. Acta Neurochir (Wien). 2015;157:1683–96. https://doi.org/10.1007/s00701-015-2512-7.
Boudreau R, Johnson M, Veile R, et al. Impact of tranexamic acid on coagulation and inflammation in murine models of traumatic brain injury and hemorrhage. J Surg Res. 2017;215:47–54. https://doi.org/10.1016/j.jss.2017.03.031.
CRASH-2 trial collaborators, Shakur H, Roberts I, Bautista R, et al. Effects of tranexamic acid on death, vascular occlusive events, and blood transfusion in trauma patients with significant haemorrhage (CRASH-2): a randomised, placebo-controlled trial. Lancet 2010; 376 (9734): 23–32. https://doi.org/10.1016/S0140-6736(10)60835-5.
Roberts I. Shakur H, Coats T, et al. The CRASH-2 trial: a randomised controlled trial and economic evaluation of the effects of tranexamic acid on death, vascular occlusive events and transfusion requirement in bleeding trauma patients. Health Technol Assess. 2013;17(10):1–79. https://doi.org/10.3310/hta17100.
CRASH-2 trial collaborators, Roberts I, Shakur H, Afolabi A, et al. The importance of early treatment with tranexamic acid in bleeding trauma patients: an exploratory analysis of the CRASH-2 randomised controlled trial. Lancet 2011;377(9771):1096–101. https://doi.org/10.1016/S0140-6736(11)60278-X (1101 e1091-2)
Majima N, Nishihara I, Yamaguchi K, et al. Usefulness of tranexamic acid in patients with severe head injury. Masui. 2013;62:410–5 (PMID: 23697191).
Mahmood A, Roberts I, Shakur H. A nested mechanistic sub-study into the effect of tranexamic acid versus placebo on intracranial haemorrhage and cerebral ischaemia in isolated traumatic brain injury: study protocol for a randomised controlled trial (CRASH-3 Trial Intracranial Bleeding Mechanistic Sub-Study [CRASH-3 IBMS]). Trials. 2017;18:330. https://doi.org/10.1186/s13063-017-2073-6.
Mahmood A, Roberts I, Shakur H. Does tranexamic acid improve outcomes in traumatic brain injury? BMJ. 2016;354:i4814. https://doi.org/10.1136/bmj.i4814.
Morrison JJ, Dubose JJ, Rasmussen TE, et al. Military application of tranexamic acid in trauma emergency resuscitation (MATTERs) study. Arch Surg. 2012;147:113–9. https://doi.org/10.1001/archsurg.2011.287.
Dewan Y, Komolafe EO, Mejia-Mantilla JH, et al. CRASH-3-tranexamic acid for the treatment of significant traumatic brain injury: study protocol for an international randomized, double-blind, placebo-controlled trial. Trials. 2012;13:87. https://doi.org/10.1186/1745-6215-13-87.
Napolitano LM, Cohen MJ, Cotton BA, et al. Tranexamic acid in trauma. J Trauma Acute Care Surg. 2013;74:1575–86. https://doi.org/10.1097/TA.0b013e318292cc54.
Yutthakasemsunt S, Kittiwatanagul W, Piyavechvirat P, et al. Tranexamic acid for patients with traumatic brain injury: a randomized, double-blinded, placebo-controlled trial. BMC Emerg Med. 2013;13:20. https://doi.org/10.1186/1471-227X-13-20.
Perel P, Al-Shahi Salman R, Kawahara T, Morris Z, Prieto-Merino D, Roberts I, et al. CRASH-2 (Clinical Randomisation of an Antifibrinolytic in Significant Haemorrhage) intracranial bleeding study: the effect of tranexamic acid in traumatic brain injury a nested randomised, placebo-controlled trial. Health Technol Assess. 2012;16(13):iii–xii. https://doi.org/10.3310/hta16130 (1–54).
Gayet-Ageron A, Prieto-Merino D, Ker K,et al. Effect of treatment delay on the effectiveness and safety of antifibrinolytics in acute severe haemorrhage: a meta-analysis of individual patient-level data from 40138 bleeding patients. Lancet. 2018;391(10116):125–32. https://doi.org/10.1016/S0140-6736(17)32455-8.
Ker K, Roberts I, Shakur H, Coats TJ. Antifibrinolytic drugs for acute traumatic injury (Review). Cochrane Database Syst Rev. 2015;9:CD004896. https://doi.org/10.1002/14651858.CD004896.pub4.
Roberts I. Tranexamic acid in trauma: how should we use it? J Thromb Haemost. 2015;13(Suppl 1):S195–9. https://doi.org/10.1111/jth.12878.
Jennett B, Bond M. Assessment of outcome after severe brain damage. Lancet. 1975;1(7905):480–4.
Hanley JA, McNeil BJ. The meaning and use of the area under a receiver operating characteristic (ROC) curve. Radiology. 1982;143(1):29–36.
Nakae R, Takayama Y, Kuwamoto K, et al. Time course of coagulation and fibrinolytic parameters in patients with traumatic brain injury. J Neurotrauma. 2016;33(7):688–95. https://doi.org/10.1089/neu.2015.4039.
Harhangi BS, Kompanje EJO, Leebeek FWG, et al. Coagulation disorders after traumatic brain injury. Acta Neurochir (Wien). 2008;150:165–75. https://doi.org/10.1007/s00701-007-1475-8.
CRASH-2 Collaborators. Intracranial Bleeding Study. Effect of tranexamic acid in traumatic brain injury: a nested randomised, placebo controlled trial (CRASH-2 Intracranial Bleeding Study). BMJ. 2011;343:d3795. https://doi.org/10.1136/bmj.d3795.
French KF, White J, Hoesch RE. Treatment of intracerebral hemorrhage with tranexamic acid after thrombolysis with tissue plasminogen activator. Neurocrit Care. 2012;17(1):107–11. https://doi.org/10.1007/s12028-012-9681-5.
Zehtabchi S, Abdel Baki SG, Falzon L, et al. Tranexamic acid for traumatic brain injury: a systematic review and meta-analysis. Am J Emerg Med. 2014;32:1503–9. https://doi.org/10.1016/j.ajem.2014.09.023.
Fakharian E, Abedzadeh-kalahroudi M, Atoof F. Effect of tranexamic acid on prevention of hemorrhagic mass growth in patients with traumatic brain injury. World Neurosurg. 2018;109:e748–53. https://doi.org/10.1016/j.wneu.2017.10.075.
Valle EJ, Allen CJ, Van Haren RM, et al. Do all trauma patients benefit from tranexamic acid? J Trauma Acute Care Surg. 2014;76:1373–8. https://doi.org/10.1097/TA.0000000000000242.
Jokar A, Ahmadi K, Salehi T, et al. The effect of tranexamic acid in traumatic brain injury: a randomized controlled trial. Chin J Traumatol. 2017;20(1):49–51. https://doi.org/10.1016/j.cjtee.2016.02.005.
Roberts I, Edwards P, Joshi M, et al. Tranexamic acid in bleeding trauma patients: an exploration of benefits and harms. Trials. 2017;18:48. https://doi.org/10.1186/s13063-016-1750-1.
Ker K, Roberts I, Shakur H, et al. Antifibrinolytic drugs for acute traumatic injury (Review). Cochrane Database Syst Rev. 2015;9:CD004896. https://doi.org/10.1002/14651858.CD004896.pub4.
Schöchl H, Schlimp CJ, Maegele M. Tranexamic acid, fibrinogen concentrate, and prothrombin complex concentrate: data to support prehospital use? Shock. 2014;41(Suppl 1):44–6. https://doi.org/10.1097/SHK.0000000000000093.
Kageyama H, Toyooka T, Tsuzuki N, Oka K. Nonsurgical treatment of chronic subdural hematoma with tranexamic acid. J Neurosurg. 2013;119(2):332–7. https://doi.org/10.3171/2013.3.JNS122162.
Funding
None.
Author information
Authors and Affiliations
Contributions
Study concept and design (OCW, KCH); acquisition of the data (AS, AT, JM, AN, HK, BS); analysis of the data (OCW); drafting of the manuscript (OCW, AS, AN); critical revision of the manuscript (OCW, MB, NR); approval of final manuscript (OCW, NR).
Corresponding author
Ethics declarations
Conflict of interest
Olfa Chakroun-Walha, Amal Samet, Mouna Jerbi, Abdennour Nasri, Aziza Talbi, Hassen Kanoun, Basma Souissi, Kamilia Chtara, Mounir Bouaziz, Hichem Ksibi and Noureddine Rekik declare that they have no competing interest.
Rights and permissions
About this article

Cite this article
Chakroun-Walha, O., Samet, A., Jerbi, M. et al. Benefits of the tranexamic acid in head trauma with no extracranial bleeding: a prospective follow-up of 180 patients. Eur J Trauma Emerg Surg 45, 719–726 (2019). https://doi.org/10.1007/s00068-018-0974-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00068-018-0974-z