
Abstract
Purpose
To assess whether the definition of an IHF used as an exclusion criterion influences the results of trauma center benchmarking.
Methods
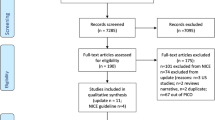
We conducted a multicenter retrospective cohort study with data from an integrated Canadian trauma system. The study population included all patients admitted between 1999 and 2010 to any of the 57 adult trauma centers. Seven definitions of IHF based on diagnostic codes, age, mechanism of injury, and secondary injuries, identified in a systematic review, were used. Trauma centers were benchmarked using risk-adjusted mortality estimates generated using the Trauma Risk Adjustment Model. The agreement between benchmarking results generated under different IHF definitions was evaluated with correlation coefficients on adjusted mortality estimates. Correlation coefficients >0.95 were considered to convey acceptable agreement.
Results
The study population consisted of 172,872 patients before exclusion of IHF and between 128,094 and 139,588 patients after exclusion. Correlation coefficients between risk-adjusted mortality estimates generated in populations including and excluding IHF varied between 0.86 and 0.90. Correlation coefficients of estimates generated under different definitions of IHF varied between 0.97 and 0.99, even when analyses were restricted to patients aged ≥65 years.
Conclusions
Although the exclusion of patients with IHF has an influence on the results of trauma center benchmarking based on mortality, the definition of IHF in terms of diagnostic codes, age, mechanism of injury and secondary injury has no significant impact on benchmarking results. Results suggest that there is no need to obtain formal consensus on the definition of IHF for benchmarking activities.
Similar content being viewed by others


References
Centers for Disease Control and Prevention. Cost of injury. 2007; Available from: http://www.cdc.gov/ncipc/factsheets/Cost_of_Injury.htm. Accessed 26 April 2007.
Sunnybrook Research Institute. The enormous human and financial cost of trauma. 2007; Available from: http://sunnybrook.ca/foundation/media/?c=11&page=23129. Accessed 12 April 2011.
Iezzoni L. Risk adjustment for measuring health care outcomes. 3rd ed. Chicago: Health Administration Press; 2003.
American College of Surgeons, National Trauma Data Bank report. 2005; Available from: http://www.facs.org/trauma/ntdb.html Accessed 27 April 2011.
Tiao J, et al. Establishing consensus on the definition of an isolated hip fracture for trauma system performance evaluation: a systematic review. J Emerg Trauma Shock. 2014;7(3):209–14.
Cudnik MT, et al. Level I versus Level II trauma centers: an outcomes-based assessment. J Trauma. 2009;66(5):1321–6.
Cudnik MT, et al. Are all trauma centers created equally? A statewide analysis. Acad Emerg Med. 2010;17(7):701–8.
American College of Surgeons, Trauma program. Resources for optimal care of the injured patient. 2006; Available from: http://www.facs.org/trauma/. Accessed 16 March 2011.
Association for Advancement of Automotive Medicine. The Abbreviated Injury Scale. 1990 Revision. Des Plaines, IL 60018, USA; 1990.
Moore L, et al. A new method for evaluating trauma centre outcome performance: TRAM-adjusted mortality estimates. Ann Surg. 2010;251(5):952–8.
Moore L, et al. The trauma risk adjustment model: a new model for evaluating trauma care. Ann Surg. 2009;249(6):1040–6.
Zar JH. Biostatistical analysis. 3rd ed. Englewood Cliffs: Prentice Hall; 1996.
Papadimitropoulos EA, et al. Current and projected rates of hip fracture in Canada. CMAJ. 1997;157(10):1357–63.
Nathens AB, et al. Relationship between trauma center volume and outcomes. JAMA. 2001;285(9):1164–71.
Parker MJ, Pryor GA. J Myles J. 11-year results in 2846 patients of the Peterborough Hip Fracture Project: reduced morbidity, mortality and hospital stay. Acta Orthop Scand. 2000;71(1):34–8.
Gomez D, et al. Hips can lie: impact of excluding isolated hip fractures on external benchmarking of trauma center performance. J Trauma. 2010;69(5):1037–41.
Bergeron E, et al. Should patients with isolated hip fractures be included in trauma registries? J Trauma. 2005;58(4):793–7.
Kuimi BL, et al. Access to a Canadian provincial integrated trauma system: a population-based cohort study. Injury. 2015;46(4):595–601.
Moore L, et al. Multiple imputation of the Glasgow Coma Score. J Trauma. 2005;59(3):698–704.
Moore L, et al. Evaluating the validity of multiple imputation for missing physiological data in the national trauma data bank. J Emerg Trauma Shock. 2009;2(2):73–9.
Conflict of interest
Tiao J, Moore L, Porgo TV, and Belcaid A declare that they have no conflict of interest.
Ethical standards
All procedures performed in the study involving human participants were in accordance with the ethical standards of the institutional ethics committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. For this type of study, formal consent is not required. This article does not contain any studies with animals performed by any of the authors.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Tiao, J., Moore, L., Porgo, T.V. et al. Evaluation of the influence of the definition of an isolated hip fracture as an exclusion criterion for trauma system benchmarking: a multicenter cohort study. Eur J Trauma Emerg Surg 42, 345–350 (2016). https://doi.org/10.1007/s00068-015-0542-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00068-015-0542-8