
Abstract
Background:
The triage of trauma patients is currently based on the trauma mechanism. However, it is known that elderly patients can sustain severe injuries due to insignificant trauma mechanisms. As such, triage methods might be questionable.
Objective:
To evaluate whether current trauma triage criteria are appropriate in severely injured elderly patients.
Methods:
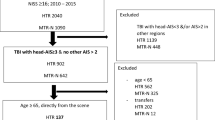
To analyze the effect of the trauma mechanism on triage and treatment, consecutive patients ≥ 55 years of age, with an injury severity score > 15, treated from 2002 to 2005 were divided into those who sustained a high-energy trauma (HET) versus a low energy trauma (LET). Pre-hospital and in-hospital data, injury characteristics, and data on mortality and disablement one year postinjury (sickness impact profile) were analyzed for HET and LET groups.
Results:
Age, sex and co-morbidity rate were similar in 84 HET patients and 107 LET patients. HET patients (mean ISS 28) received more sophisticated trauma care than LET patients (mean ISS 22), although mortality was similar (38 vs. 34%). Long-term disablement was also similar (median SIP scores 4 vs. 6). Severe head injuries and the Revised Trauma Score were related to mortality. Physical disablement was related to preexisting co-morbidities. No variables were related to psychosocial disablement.
Conclusions:
In elderly people a low energy trauma may lead to severe consequences. Not only the trauma mechanism, but also age, co-morbidity, and the likelihood of a brain injury should be leading in the triage and subsequent management of severely injured elderly.
Similar content being viewed by others


References
Nijboer JMM, van der Sluis CK, van der Naalt J, Two cohorts of severely injured trauma patients, nearly two decades apart: unchanged mortality but improved quality of life despite higher age. J Trauma 2007;63:670–5.
Champion HR, Copes WS, Buyer D, et al. Major trauma in geriatric patients. Am J Public Health 1989;79:1278–82.
Lonner JH, Koval KJ. Polytrauma in the elderly. Clin Orthop 1995;318:136–43.
Kilaru S, Garb J, Emhoff T, et al. Long-term functional status and mortality of elderly patients with severe closed head injuries. J Trauma 1996;41:957–63.
Finelli FC, Jonsson J, Champion HR, et al. A case control study for major trauma in geriatric patients. J Trauma 1989;29:541–8.
Kuhne CA, Ruchholtz S, Kaiser GM, et al. Mortality in severely injured elderly trauma patients-when does age become a risk factor? Word J Surg 2005;29:1476–82.
Shabot MM, Johnson CL. Outcome from critical care in the oldest old trauma patients. J Trauma 1995;39:254–9.
Scalea TM, Simon HM, Duncan AO, et al. Geriatric blunt trauma: improved survival with early invasive monitoring. J Trauma 1990;30:129–34.
American College of Surgeons Committee on Trauma (2000) (Amendments to) Resources for Optimal Care of the Injured Patient: 2000. Chicago: American College of Surgeons.
Velmahos GC, Jindal A, Chan LS, et al. Insignificant mechanism of injury: not to be taken lightly. J Am Coll Surg 2001;192:147–52.
Helling TS, Watkins M, Evans LL, et al. Low falls: an underappreciated mechanism of injury. J Trauma 1999;46:453–6.
Sterling DA, O’Connor JA, Bonadies J. Geriatric falls: injury severity is high and disproportionate to mechanism. J Trauma 2001;50:116–9.
Phillips S, Rond PC, Kelly S, et al. The failure of triage criateria to identify geriatric patients with trauma: results from the Florida Trauma Triage Study. J Trauma 1996;40:278–83.
The Abbreviated Injury Scale (1998) 1990 revision, updated. Association for the Advancement of Automotive Medicine, Des Plaines, IL.
Jennett B, Bond M. Assessment of outcome after severe brain damage. Lancet 1975;1:480–4.
Bergner M, Bobbitt RA, Carter WB, et al. The SIP: development and final revision of a health status measure. Med Care 1981;19:787–805.
Jurkovich G, Mock C, MacKenzie E, et al. The Sickness Impact Profile as a tool to evaluate functional outcome in trauma patients. J Trauma 1995;39:625–31.
Jacobs HM, Luttik A, Touw-Otten FWMM, et al. De ’sickness impact profile’; resultaten van een valideringsonderzoek van de Nederlandse versie. Ned Tijdschr Geneesk 1990;134:1950–4.
Rodin G, Voshart K. Depressive symptoms and functional impairment in the medically ill. Gen Hosp Psychiat 1987;9:251–8.
Boyd CR, Tolson MA, Copes WS. Evaluating trauma care: the TRISS model. J Trauma 1987;27:370–8.
Sampalis JS, Denis R, Frechette P, et al. Direct transport to tertiary trauma centers versus transfer from lower level facilities: impact on mortality and morbidity among patients with major trauma. J Trauma 1997;43:288–96.
Ma MH, MacKenzie EJ, Alcorta R, et al. Compliance with prehospital triage protocol for major trauma patients. J Trauma 1999;46:168–75.
Ochsner MG, Schmidt JA, Rozycki GS, et al. The evaluation of a two-tier trauma response system at a major trauma center: is it cost effective and safe? J Trauma 1995;39:971–7.
Oreskovich MR, Howard J, Copass MK, et al. Geriatric trauma: injury patterns and outcome. J Trauma 1984;24:565–9.
Sartorelli KH, Rogers FB, Osler TM, et al. Financial aspects of providing trauma care at the extremes of age. J Trauma 1999;46:483–7.
Demetriades D, Karaiskakis M, Velmahos G, et al. Effect on outcome of early intensive mamagement of geriatric trauma patients. Br J Surg 2002;89:1319–22.
Battistella FD, Din AM, Perez L. Trauma patients 75 years and older: long-term follow-up results justify aggressive management. J Trauma 1998;44:618–24.
van der Sluis CK, Klasen HJ, Eisma WH, et al. Major trauma in young and old: what is the difference? J Trauma 1996;40:78–82.
Jacobs DG, Plaisier BR, Barie PS, et al. Practice management guidelines for geriatric trauma: the EAST practice management guidelines work group. J Trauma 2003;54:391–416.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Nijboer, J.M.M., van der Sluis, C.K., Dijkstra, P.U. et al. The Value of the Trauma Mechanism in the Triage of Severely Injured Elderly. Eur J Trauma Emerg Surg 35, 49–55 (2009). https://doi.org/10.1007/s00068-008-7069-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00068-008-7069-1