
Abstract
Purpose
The goal of this work was to investigate the oncological outcome of whole pelvis radiotherapy (wpRT) in pathologic pelvic lymph node-positive (pN1) prostate cancer (PCa), evaluate the location of relapse, and identify potential prognostic factors.
Patients and methods
All patients undergoing pelvic lymph node dissection (PLND) since the year 2000 at a single tertiary care center were evaluated. A total of 154 patients with pN1 PCa were treated with wpRT (39 in an adjuvant setting) and 2–3 years of androgen deprivation therapy (ADT). Kaplan–Meier analysis was performed to estimate biochemical recurrence-free survival (bRFS), clinical progression-free survival (cPFS), and prostate cancer-specific survival (CSS). Uni- and multivariate regression analyses were performed to identify prognostic factors.
Results
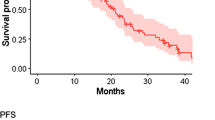
Estimated bRFS was 67%, cPFS was 71%, and CSS was 96% at 5 years. Median follow-up was 55 months (interquartile range 25–87). Multivariate analysis identified having only 1 positive lymph node, a shorter time between diagnosis and PLND, and older age as independent favorable prognostic factors for biochemical and clinical recurrence. The number of positive lymph nodes was prognostic for CSS (hazard ratio [HR] 1.34, 95% confidence interval 1.17–1.54) and OS (HR 1.22, 95% confidence interval 1.10–1.36). Bone metastases were the most frequent location of PCa relapse (n = 32, 64%).
Conclusions
Patients with pN1 PCa treated with wpRT and 2–3 years ADT have an encouraging 5‑year CSS. Understaging of the disease extent may be the most important enemy in definitive pN1 PCa treatment.
Zusammenfassung
Ziel
Das Ziel dieser Studie war es, das onkologische Outcome der Bestrahlung des gesamten Beckens (wpRT) beim histologisch gesicherten nodal metastasierten Prostatakarzinom zu untersuchen, die Lokalisation eines eventuellen Rezidivs zu charakterisieren und mögliche prognostische Faktoren zu identifizieren.
Methoden
Alle Patienten, bei denen seit dem Jahr 2000 eine pelvine Lymphknotendissektion (PLND) durchgeführt worden war, wurden eingeschlossen. Insgesamt 154 Patienten mit pN1-Prostatakarzinomen wurden mit wpRT (davon 39 im adjuvanten Setting) und Androgendeprivation (ADT) behandelt. Zur Bestimmung des biochemischen rezidivfreien Intervalls (bRFS), des klinischen progressionsfreien Überlebens (cPFS) und des Prostatakarzinom-spezifischen Gesamtüberlebens (CSS) wurden Kaplan-Meier-Analysen durchgeführt. Mögliche prognostische Faktoren wurden mittels uni- und multivariater Regressionsanalyse identifiziert.
Ergebnisse
Das bRFS wurde für ein Beobachtungsintervall von 5 Jahren auf 67 %, das cPFS auf 71 % und die CSS auf 96 % geschätzt. Das mediane Follow-up betrug 55 Monate (IQR 25–87). Nur 1 positiver Lymphknoten, eine kurze Zeit zwischen Diagnose und PLND und höheres Alter waren in der multivariaten Analyse günstige prognostische Faktoren bezüglich eines biochemischen oder klinischen Rezidivs. Die Anzahl der positiven Lymphknoten war ein prognostischer Faktor für das CSS (HR 1,34 [1,17–1,54]) und das Gesamtüberleben (HR 1,22 [1,10–1,36]). Das Achsenskelett war die häufigste Lokalisation eines PCa-Rezidivs (n = 32, 64 %).
Schlussfolgerung
Das 5‑Jahres-CSS bei Patienten mit nodal metastasiertem Prostatakarzinom, die mit wpRT und 2–3 Jahren ADT behandelt werden, ist erfreulich hoch. Die Unterschätzung des Ausmaßes der Erkrankung könnte der wesentlichste adverse Faktor bezüglich einer guten Langzeitprognose bei der Behandlung von Patienten mit nodal metastasiertem Prostatakarzinom darstellen.


Similar content being viewed by others


References
Messing EM, Manola J, Yao J, Kiernan M, Crawford D, Wilding G et al (2006) Immediate versus deferred androgen deprivation treatment in patients with node-positive prostate cancer after radical prostatectomy and pelvic lymphadenectomy. Lancet Oncol 7:472–479. doi:10.1016/S1470-2045(06)70700-8
Aus G, Nordenskjöld K, Robinson D, Rosell J, Varenhorst E (2003) Prognostic factors and survival in node-positive (N1) prostate cancer – a prospective study based on data from a Swedish population-based cohort. Eur Urol 43:627–631. doi:10.1016/S0302-2838(03)00156-8
Engel J, Bastian PJ, Baur H, Beer V, Chaussy C, Gschwend JE et al (2010) Survival benefit of radical prostatectomy in lymph node – positive patients with prostate cancer. Eur Urol 57:754–761. doi:10.1016/j.eururo.2009.12.034
Steuber T, Budäus L, Walz J, Zorn KC, Schlomm T, Chun F et al (2011) Radical prostatectomy improves progression-free and cancer-specific survival in men with lymph node positive prostate cancer in the prostate-specific antigen era: a confirmatory study. BJU Int 107:1755–1761. doi:10.1111/j.1464-410X.2010.09730.x
Ghavamian R, Bergstralh EJ, Blute ML, Slezak J, Zincke H (1999) Radical retropubic prostatectomy plus orchiectomy versus orchiectomy alone for pTxN+ prostate cancer: a matched comparison. J Urol 161:1223–1227. doi:10.1016/S0022-5347(01)61640-9
James ND, Spears MR, Clarke NW, Dearnaley DP, Mason MD, Parker CC et al (2015) Failure-free survival and radiotherapy in patients with newly diagnosed nonmetastatic prostate cancer: data from patients in the control arm of the STAMPEDE trial. JAMA Oncol 2:348–357. doi:10.1001/jamaoncol.2015.4350
Lawton CA, Winter K, Grignon D, Pilepich MV (2005) Androgen suppression plus radiation versus radiation alone for patients with stage D1/pathologic node-positive adenocarcinoma of the prostate: updated results based on national prospective randomized trial Radiation Therapy Oncology Group 85–31. J Clin Oncol 23:800–807. doi:10.1200/JCO.2005.08.141
Gakis G, Boorjian SA, Briganti A, Joniau S, Karazanashvili G, Karnes RJ et al (2014) The role of radical prostatectomy and lymph node dissection in lymph node–positive prostate cancer: a systematic review of the literature. Eur Urol 66:191–199. doi:10.1016/j.eururo.2013.05.033
Lilleby W, Narrang A, Tafjord G, Vlatkovic L, Russnes KM, Stensvold A et al (2015) Favorable outcomes in locally advanced and node positive prostate cancer patients treated with combined pelvic IMRT and androgen deprivation therapy. Radiat Oncol 10:232. doi:10.1186/s13014-015-0540-3
Robnett TJ, Whittington R, Malkowicz SB, Brereton HD, Van Arsdalen K, Drach G et al (2002) Long-term use of combined radiation therapy and hormonal therapy in the management of Stage D1 prostate cancer. Int J Radiat Oncol Biol Phys 53:1146–1151. doi:10.1016/S0360-3016(02)02868-7
Pinkawa M, Piroth MD, Holy R, Djukic V, Klotz J, Krenkel B et al (2011) Combination of dose escalation with technological advances (intensity-modulated and image-guided radiotherapy) is not associated with increased morbidity for patients with prostate cancer. Strahlenther Onkol 187:479–484. doi:10.1007/s00066-011-2249-z
Bolla M, de Reijke TM, Van Tienhoven G, Van den Bergh ACM, Oddens J, Poortmans PMP et al (2009) Duration of androgen suppression in the treatment of prostate cancer. N Engl J Med 360:2516–2527. doi:10.1056/NEJMoa0810095
Briganti A, Karnes RJ, Da Pozzo LF, Cozzarini C, Capitanio U, Gallina A et al (2011) Combination of adjuvant hormonal and radiation therapy significantly prolongs survival of patients with pT2–4 pN+ prostate cancer: results of a matched analysis. Eur Urol 59:832–840. doi:10.1016/j.eururo.2011.02.024
Dorff TB, Flaig TW, Tangen CM, Hussain MHA, Swanson GP, Wood DP et al (2011) Adjuvant androgen deprivation for high-risk prostate cancer after radical prostatectomy: SWOG S9921 study. J Clin Oncol 29:2040–2045. doi:10.1200/JCO.2010.32.2776
Haglind E, Carlsson S, Stranne J, Wallerstedt A, Wilderäng U, Thorsteinsdottir T et al (2015) Urinary incontinence and erectile dysfunction after robotic versus open radical prostatectomy: a prospective, controlled, nonrandomised trial. Eur Urol 68:216–225. doi:10.1016/j.eururo.2015.02.029
Roach M, Marquez C, Yuo HS, Narayan P, Coleman L, Nseyo UO et al (1994) Predicting the risk of lymph node involvement using the pre-treatment prostate specific antigen and Gleason score in men with clinically localized prostate cancer. Int J Radiat Oncol Biol Phys 28:33–37
Fonteyne V, De Gersem W, De Neve W, Jacobs F, Lumen N, Vandecasteele K et al (2009) Hypofractionated intensity-modulated arc therapy for lymph node metastasized prostate cancer. Int J Radiat Oncol Biol Phys 75:1013–1020. doi:10.1016/j.ijrobp.2008.12.047
Decaestecker K, De Meerleer G, Ameye F, Fonteyne V, Lambert B, Joniau S et al (2014) Surveillance or metastasis-directed therapy for oligometastatic prostate cancer recurrence (STOMP): study protocol for a randomized phase II trial. BMC Cancer 14:671. doi:10.1186/1471-2407-14-671
Epstein JI, Zelefsky MJ, Sjoberg DD, Nelson JB, Egevad L, Magi-Galluzzi C et al (2016) A contemporary prostate cancer grading system: a validated alternative to the Gleason score. Eur Urol 69:428–435. doi:10.1016/j.eururo.2015.06.046
Da Pozzo LF, Cozzarini C, Briganti A, Suardi N, Salonia A, Bertini R et al (2009) Long-term follow-up of patients with prostate cancer and nodal metastases treated by pelvic lymphadenectomy and radical prostatectomy: the positive impact of adjuvant radiotherapy. Eur Urol 55:1003–1011. doi:10.1016/j.eururo.2009.01.046
Abdollah F, Karnes RJ, Suardi N, Cozzarini C, Gandaglia G, Fossati N et al (2014) Impact of adjuvant radiotherapy on survival of patients with node-positive prostate cancer. J Clin Oncol 32:3939–3947. doi:10.1200/JCO.2013.54.7893
Whittington R, Malkowicz SB, Machtay M, Van Arsdalen K, Barnes MM, Broderick GA et al (1997) The use of combined radiation therapy and hormonal therapy in the management of lymph node-positive prostate cancer. Int J Radiat Oncol Biol Phys 39:673–680. doi:10.1016/S0360-3016(97)00369-6
Mottet N, Bellmunt J, Wiegel T (2016) EAU Guidelines on Prostate Cancer 2016. https://uroweb.org/guideline/prostate-cancer/. Accessed May 1, 2016
Abdollah F, Gandaglia G, Suardi N, Capitanio U, Salonia A, Nini A et al (2015) More extensive pelvic lymph node dissection improves survival in patients with node-positive prostate cancer. Eur Urol 67:212–219. doi:10.1016/j.eururo.2014.05.011
Daneshmand S, Quek ML, Stein JP, Lieskovsky G, Cai J, Pinski J et al (2004) Prognosis of patients with lymph node positive prostate cancer following radical prostatectomy: long-term results. J Urol 172:2252–2255. doi:10.1097/01.ju.0000143448.04161.cc
Passoni NM, Abdollah F, Suardi N, Gallina A, Bianchi M, Tutolo M et al (2014) Head-to-head comparison of lymph node density and number of positive lymph nodes in stratifying the outcome of patients with lymph node-positive prostate cancer submitted to radical prostatectomy and extended lymph node dissection. Urol Oncol 32(29):e21–e28. doi:10.1016/j.urolonc.2012.10.009
Briganti A, Karnes JR, Da Pozzo LF, Cozzarini C, Gallina A, Suardi N et al (2009) Two positive nodes represent a significant cut-off value for cancer specific survival in patients with node positive prostate cancer. A new proposal based on a two-institution experience on 703 consecutive N+ patients treated with radical prostatectomy. Eur Urol 55:261–270. doi:10.1016/j.eururo.2008.09.043
Schumacher MC, Burkhard FC, Thalmann GN, Fleischmann A, Studer UE (2008) Good outcome for patients with few lymph node metastases after radical retropubic prostatectomy. Eur Urol 54:344–352. doi:10.1016/j.eururo.2008.05.023
Seiler R, Studer UE, Tschan K, Bader P, Burkhard FC (2014) Removal of limited nodal disease in patients undergoing radical prostatectomy: long-term results confirm a chance for cure. J Urol 191:1280–1285. doi:10.1016/j.juro.2013.11.029
Bosco C, Crawley D, Adolfsson J, Rudman S, Van Hemelrijck M (2015) Quantifying the evidence for the risk of metabolic syndrome and its components following androgen deprivation therapy for prostate cancer: a meta-analysis. PLOS ONE 10:e0117344. doi:10.1371/journal.pone.0117344
Van Hemelryk A, De Meerleer G, Ost P, Poelaert F, De Gersem W, Decaestecker K et al (2016) The outcome for patients with pathologic node-positive prostate cancer treated with intensity modulated radiation therapy and androgen deprivation therapy: a case-matched analysis of pN1 and pN0 patients. Int J Radiat Oncol Biol Phys 96:323–332. doi:10.1016/j.ijrobp.2016.06.011
Chang L, Graham PH, Hao J, Bucci J, Cozzi PJ, Kearsley JH et al (2014) Emerging roles of radioresistance in prostate cancer metastasis and radiation therapy. Cancer Metastasis Rev 33:469–496. doi:10.1007/s10555-014-9493-5
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
F. Poelaert, V. Fonteyne, P. Ost, B. De Troyer, K. Decaestecker, G. De Meerleer, P. De Visschere, T. Claeys, B. Dhondt, and N. Lumen declare that they have no competing interests.
Ethical standards
This retrospective study was approved by the local ethics committee (UZG2011/495).
Caption Electronic Supplementary Material
66_2016_1094_MOESM2_ESM.doc
Table 2 Multivariate Cox regression analysis for outcome, with different steps to identify independent prognostic factors
Rights and permissions
About this article

Cite this article
Poelaert, F., Fonteyne, V., Ost, P. et al. Whole pelvis radiotherapy for pathological node-positive prostate cancer. Strahlenther Onkol 193, 444–451 (2017). https://doi.org/10.1007/s00066-016-1094-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00066-016-1094-5