
Background and Purpose:
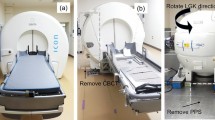
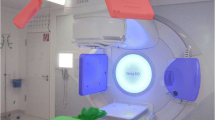
Modern medical linear accelerators (linacs) are equipped with X-ray systems, which allow to check the patient’s position just prior to treatment. Their usefulness for stereotactic radiosurgery (SRS) depends on how accurately they allow to determine the deviation between the actual and planned isocenter positions. This accuracy was investigated with measurements using two different phantoms (Figures 1 and 2).
Material and Methods:
After precisely aligning a phantom onto the linac isocenter, two perpendicular X-rays or a cone-beam CT (CBCT) are taken, and the isocenter position is deduced from this data. The deviation of the thereby gained position from the setup isocenter is taken as a measure for the uncertainty of this method.
Results:
Isocenter verification with two orthogonal X-rays (Figure 4) achieves accuracies of better than 1 mm (Table 3). The distance between the isocenters of the CBCT and the linac (Figure 3) is in the order of 1 mm, but remains constant on the time scale of 1 week (Table 1) and may therefore be taken into account. The uncertainty after correction is below 0.2 mm.
Conclusion:
kV imaging with the patient in treatment position allows to verify the isocenter position with submillimeter precision, and therefore offers a supplemental test, suitable for SRS, which takes all positional uncertainties into account.
Hintergrund und Ziel:
Moderne medizinische Linearbeschleuniger (Linacs) sind mit Röntgenanlagen ausgestattet, die es erlauben, die Position des Patienten direkt vor der Behandlung zu überprüfen. Ihr Nutzen für die stereotaktische Radiochirurgie (SRS) hängt davon ab, wie genau man die Abweichung zwischen der momentanen und der geplanten Isozentrumsposition bestimmen kann. Diese Genauigkeit wurde mit Messungen an zwei verschiedenen Phantomen untersucht (Abbildungen 1 und 2).
Material und Methodik:
Nach präziser Positionierung des Phantoms auf das Isozentrum des Linac werden zwei orthogonale Röntgenbilder oder ein „cone-beam“-CT (CBCT) aufgenommen, aus denen die Isozentrumsposition bestimmt wird. Die Abweichung der so ermittelten Position vom eingestellten Isozentrum wird als Maß für die Ungenauigkeit der Methode angenommen.
Ergebnisse:
Isozentrumskontrolle mit zwei orthogonlen Röntgenaufnahmen (Abbildung 4) erreicht eine Genauigkeit von besser als 1 mm (Tabelle 3). Der Abstand zwischen den Isozentren des CBCT und des Linac (Abbildung 3) liegt in der Größenordnung von 1 mm, bleibt aber während 1 Woche konstant (Tabelle 1) und kann somit berücksichtigt werden. Die Ungenauigkeit nach dieser Korrektur ist unterhalb von 0,2 mm.
Schlussfolgerung:
kV-Bildgebung mit dem Patienten in der Behandlungsposition erlaubt eine Isozentrumskontrolle mit Submillimeterpräzision und bietet damit einen zusätzlichen Test, der für die SRS geeignet ist und alle räumlichen Unsicherheiten berücksichtigt.
Similar content being viewed by others

References
Chang J, Yenice K, Narayana A, et al. Accuracy and feasibility of cone-beam computed tomography for stereotactic radiosurgery setup. Med Phys 2007;34:2077–84.
Debus J, Pirzkall A, Schlegel W, et al. Stereotaktische Einzeitbestrahlung (Radiochirurgie). Strahlenther Onkol 1999;175:47–56.
Feldkamp L, Davis L, Kress J. Practical cone-beam algorithm. Int J Optical Soc Am A 1984;1:612–9.
Geyer P, Blank H, Evers C, et al. Filmless evaluation of the mechanical accuracy of the isocenter in stereotactic radiotherapy. Strahlenther Onkol 2007;183:76–80.
Guckenberger M, Baier K, Guenther I, et al. Reliability of the bony anatomy in image-guided stereotactic radiotherapy of brain metastases. Int J Radiat Oncol Biol Phys 2007;69:294–301.
Guckenberger M, Meyer J, Wilbert J, et al. Cone-beam CT-based image guidance for extracranial stereotactic radiotherapy of intrapulmonary tumors. Acta Oncol 2006;45:897–906.
Hartmann G, Bauer-Kirpes B, Serago C, et al. Precision and accuracy of stereotactic convergent beam irradiations from a linear accelerator. Int J Radiat Oncol Biol Phys 1994;28:481–92.
Hristov D, Fallone B. A grey-value image alignment algorithm for registration of portal images and digitally reconstructed radiographs. Med Phys 1996;23:75–84.
Jin JY, Ryu S, Faber K, et al. 2D/3D image fusion for accurate target localization and evaluation of a mask based stereotactic system in fractionated stereotactic radiotherapy of cranial lesions. Med Phys 2006;33:4557–66.
Koehler F, Boda-Heggemann J, Kuepper B, et al. Accuracy of a commercially available algorithm for multiple-fiducial-based grey value matching by cone-beam CT. Strahlenther Onkol 2008;184:Special Issue 2:96.
Mack A, Mack G, Weltz D, et al. Qualitätssicherung im stereotaktischen Raum. Bestimmung der Genauigkeit von Ort und Dosis bei Ein-Zeit-Bestrahlungen. Strahlenther Onkol 2003;179:760–6.
Meyer J, Wilbert J, Baier K, et al. Positioning accuracy of cone-beam computed tomography in combination with a hexapod robot treatment table. Int J Radiat Oncol Biol Phys 2007;67:1220–8.
Oldham M, Létourneau D, Watt L, et al. Cone-beam-CT guided radiation therapy: a model for on-line application. Radiother Oncol 2005;75: 271.e1–8.
Polat B, Wilbert J, Baier K, et al. Nonrigid patient setup errors in the head and neck region. Strahlenther Onkol 2007;183:506–11.
Schell MC, Bova FJ, Larson DA, et al. Stereotactic radiosurgery. AAPM Rep 1995;54:1–88.
Serago C, Lewin A, Houdek P, et al. Stereotactic target point verification of an x ray and CT localizer. Int J Radiat Oncol Biol Phys 1991;20:517–23.
Siddon R, Barth N. Stereotactic localization of intracranial targets. Int J Radiat Oncol Biol Phys 1987;13:1241–6.
Special radiotherapy equipments — part 1: Percutaneous stereotactic radiotherapy, basic performance characteristics and essential test methods. DIN 2004;6875-1:1–32.
Special radiotherapy equipments — part 2: Percutaneous stereotactic radiotherapy, constancy testing. DIN 2008;6875-2:1–16.
Wiehle R, Hodapp N, Grosu A L. Isozentrumskontrolle für die Linac-Radiochirurgie mittels kV-Bildgebung am Beschleuniger. Strahlenther Onkol 2008;184:Sondernr 1:104–5.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Wiehle, R., Koth, HJ., Nanko, N. et al. On the Accuracy of Isocenter Verification with kV Imaging in Stereotactic Radiosurgery. Strahlenther Onkol 185, 325–330 (2009). https://doi.org/10.1007/s00066-009-1871-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00066-009-1871-5