
Purpose:
To compare radio(chemo)therapy with 41.4–50.4 Gy (moderate dose, MD-RCT) plus resection versus radio(chemo)therapy with 59.4–66.6 Gy (higher dose, HD-RCT) alone for outcome in stage III esophageal cancer, and to investigate potential prognostic factors including preradiotherapy (pre-RT) hemoglobin.
Patients and Methods:
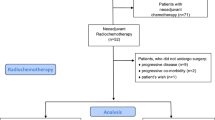
148 patients with stage III esophageal cancer, treated with MD-RCT plus resection (n = 41) or HD-RCT alone (n = 107), were retrospectively evaluated for age, gender, performance status, tumor location, tumor length, stage, histology, grading, number of chemotherapy courses, pre-RT hemoglobin, resection, overall survival (OS), metastases-free survival (MFS), and locoregional control (LC).
Results:
On univariate analysis, MD-RCT plus resection resulted in better 2-year OS (57% vs. 25%; p = 0.049), 2-year MFS (71% vs. 39%; p = 0.041), and 2-year LC (76% vs. 39%; p = 0.003). On multivariate analysis, results maintained significance for LC (p = 0.021). According to multivariate analysis, pre-RT hemoglobin was associated with OS (p = 0.003), MFS (p = 0.043), and LC (p = 0.041), tumor length with OS (p = 0.002) and MFS (p = 0.017), and the number of chemotherapy courses with OS (p = 0.008). Complications were more frequent in the MD-RCT-plus-surgery group (p < 0.001). Acute (p = 0.47) and late toxicity (p = 0.86) were similar in both groups.
In patients receiving surgery, R0 resection was superior to R1/2 resection for OS (p < 0.001), MFS (p = 0.030), and LC (p < 0.001). MD-RCT plus R0 resection was also superior to HD-RCT alone.
Conclusion:
MD-RCT plus resection resulted in better LC than HD-RCT alone. If R0 resection is possible, MD-RCT plus resection appears preferable, as it results in better outcome. If only R1/2 resection can be performed, HD-RCT alone appears preferable regarding outcome and the greater morbidity associated with resection.
Ziel:
Diese Studie vergleicht Radiochemotherapie mit 41,4–50,4 Gy (MD-RCT) plus Resektion mit alleiniger Radiochemotherapie mit 59,4–66,6 Gy (HD-RCT) bei der Behandlung des lokal fortgeschrittenen Ösophaguskarzinoms. Ferner werden mögliche Prognosefaktoren wie der Hämoglobinwert vor Radiotherapie (RT) untersucht.
Patienten und Methodik:
148 Patienten (Tabelle 1) mit einem Ösophaguskarzinom im Stadium III, die eine MD-RCT plus Resektion (n = 41) oder eine alleinige HD-RCT (n = 107) erhielten, wurden retrospektiv hinsichtlich Alter, Geschlecht, Allgemeinzustand, Tumorlokalisation, Tumorlange, Stadium, Histologie, Grading, Anzahl der Chemotherapiekurse, Hämoglobin vor RT, Resektionsstatus, Gesamtüberleben (OS), metastasenfreien Überlebens (MFS) und lokoregionaler Kontrolle (LC) untersucht.
Ergebnisse:
In der univariaten Analyse (Tabelle 2, Abbildungen 1 bis 3) waren 2-Jahres-OS (57% vs. 25%; p = 0,049), 2-Jahres- MFS (71% vs. 39%; p = 0,041) und 2-Jahres-LC (76% vs. 39%; p = 0,003) nach MD-RCT plus Resektion signifikant besser. In der Multivarianzanalyse (Tabelle 3) blieben die Ergebnisse für die LC signifikant (p = 0,021). Nach der Multivarianzanalyse hatte der Hämoglobinwert vor RT einen signifikanten Einfluss auf OS (p = 0,003), MFS (p = 0,043) und LC (p = 0,041), die Tumorlange auf OS (p = 0,002) und MFS (p = 0,017), die Zahl der Chemotherapiekurse auf OS (p = 0,008). Komplikationen traten nach MD-RCT plus Resektion häufiger auf (p < 0,001), Akuttoxizität (p = 0,47) und Spättoxizität (p = 0,86) waren vergleichbar (Tabellen 4 bis 6).
Die R0-Resektion war der R1-Resektion hinsichtlich OS (p < 0,001), MFS (p = 0,030) und LC (p < 0,001) überlegen (Tabelle 7). MD-RCT plus R0-Resektion führte zu besseren Ergebnissen als alleinige HD-RCT (Tabelle 8).
Schlussfolgerung:
Die MD-RCT plus Resektion führte zu besserer LC als die alleinige HD-RCT. Bei möglicher R0-Resektion erscheint die MD-RCT plus Resektion indiziert. Ist nur eine R1/2-Resektion möglich, sollte angesichts der Behandlungsergebnisse und möglicher operationsbedingter Komplikationen die alleinige HD-RCT erfolgen.
Similar content being viewed by others


Author information
Authors and Affiliations
Corresponding author
Additional information
* Parts of the data were presented (oral presentation) at the 11th Annual Meeting of the German Society of Radiation Oncology (DEGRO) in Karlsruhe, May 26–29, 2005.
Rights and permissions
About this article
Cite this article
Rades, D., Schulte, R., Yekebas, E.F. et al. Radio(chemo)therapy Plus Resection Versus Radio(chemo)therapy Alone for the Treatment of Stage III Esophageal Cancer*. Strahlenther Onkol 183, 10–16 (2007). https://doi.org/10.1007/s00066-007-1583-7
Received:
Revised:
Issue Date:
DOI: https://doi.org/10.1007/s00066-007-1583-7