
Abstract
Introduction
Hypoglycemia is a frequent and feared complication of insulin therapy on the intensive care unit (ICU). Sedated patients in particular are at risk for hypoglycemia due to the absence of clinical symptoms. Furthermore, recent studies point to a correlation between the variability of blood glucose and mortality. Therefore, continuous glucose monitoring has the potential to influence outcome due to a better control of blood glucose in critically ill patients.
Materials and methods
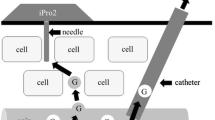
We evaluated the efficacy, accuracy and safety of a new commercially available subcutaneous continuous glucose monitoring system (sCGM; Sentrino®, Medtronic) in a pilot study in critically ill adult patients. sCGM data were recorded for up to 72 h and values were compared with blood glucose values measured by cassette-based blood gas analyzer (BGA).
Results
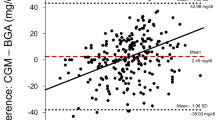
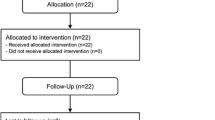
A total of 14 patients (eight male, six female), with a mean age of 62.1 ± 9.8 years, referred to the ICU after major abdominal surgery were studied. The average simplified acute physiology score (SAPS II) was 35 ± 9. Three patients had known type II diabetes. The average runtime of sensors was 44.1 ± 22.1 h. In comparison to BGA, measurement of blood glucose by sCGM revealed an accuracy of 1.5 mg/dl, and a precision of + 34.2 mg/dl to − 31.2 mg/dl. Linn’s concordance correlation coefficient yielded 0.74 with a 95 % confidence interval of 0.68–0.78. No hypoglycemic events, defined as a blood glucose level below 70 mg/dl, occurred during treatment.
Conclusions
sCGM monitoring via a subcutaneous sensor demonstrated high accuracy and considerable variability compared to blood gas samples, even in critically ill patients.
Zusammenfassung
Hintergrund
Die Hypoglykämie stellt eine häufige und gefürchtete Komplikation der Insulintherapie auf der Intensivstation dar. Insbesondere bei sedierten Patienten besteht aufgrund fehlender klinischer Symptome das Risiko einer Hypoglykämie. Außerdem weisen aktuelle Studien auf eine Korrelation zwischen der Variabilität von Blutzucker und Mortalität hin. Daher hat das kontinuierliche Glukosemonitoring das Potenzial, den Verlauf durch eine bessere Blutzuckereinstellung bei kritisch kranken Patienten zu beeinflussen.
Material und Methoden
Untersucht wurden die Wirksamkeit, Genauigkeit und Sicherheit eines neuen, kommerziell verfügbaren, subkutanen kontinuierlichen Glukosemonitoringsystems (sCGM; Sentrino®, Fa. Medtronic) in einer Pilotstudie an kritisch kranken erwachsenen Patienten. Die sCGM-Daten wurden für bis zu 72 h aufgezeichnet und die Werte mit den Blutzuckerwerten verglichen, die mittels eines kassettenbasierten Blutgasanalysators (BGA) gemessen wurden.
Ergebnisse
Es wurden insgesamt 14 Patienten (8 m, 6 w) mit einem Durchschnittsalter von 62,1 ± 9,8 Jahren untersucht, die nach einer großen Bauchoperation auf die Intensivstation verlegt wurden. Der durchschnittliche SAPS II („simplified acute physiology score“) betrug 35 ± 9. Bei 3 Patienten war ein Typ-2-Diabetes bekannt. Die durchschnittliche Nutzungsdauer der Sensoren lag bei 44,1 ± 22,1 h. Im Vergleich zur BGA ergab die Messung des Blutzuckers mit dem sCGM eine Genauigkeit von 1,5 mg/dl und eine Variabilität von + 34,2 mg/dl bis − 31,2 mg/dl. Der Konkordanz-Korrelationskoeffizient nach Linn ergab 0,74 bei einem 95 %-Konfidenzintervall von 0,68–0,78. Es traten keine Hypoglykämien, definiert als Blutzuckerspiegel unter 70 mg/dl, während der Behandlung auf.
Schlussfolgerungen
Das sCGM-Monitoring über einen subkutanen Sensor wies eine hohe Genauigkeit und eine beträchtliche Variabilität im Vergleich zu den Blutgasanalysen auf, selbst bei kritisch kranken Patienten.


Similar content being viewed by others
References
Brunkhorst FM, Engel C, Bloos F et al (2008) German Competence Network Sepsis (SepNet): intensive insulin therapy and pentastarch resuscitation in severe sepsis. N Engl J Med 358:125–139
Finfer S, Chittock DR, Su SY et al (2009) Intensive versus conventional glucose control in critically ill patients. N Engl J Med 360:1283–1297
Preiser JC, Devos P, Ruiz-Santana S et al (2009) A prospective randomised multi-centre controlled trial on tight glucose control by intensive insulin therapy in adult intensive care units: the Glucontrol study. Intensive Care Med 35:1738–1748
Egi M, Bellomo R, Stachowski E et al (2010) Hypoglycemia and outcome in critically ill patients. Mayo Clin Proc 85:217–224
Jacka MJ, Torok-Both CJ, Bagshaw SM (2009) Blood glucose control among critically ill patients with brain injury. Can J Neurol Sci 36:436–442
Finfer S (2011) Hypoglycemia in critically ill adults—association yes, causation not proven. Crit Care 15:1012
Holzinger U (2013) Glucose control in the critically ill. Innovations and contemporary strategies. Med Klin Intensivmed Notfmed 108:422–428
Egi M, Bellomo R, Stachowski E et al (2006) Variability of blood glucose concentration and short-term mortality in critically ill patients. Anesthesiology 105:244–252
Bagshaw SM, Bellomo R, Jacka MJ et al (2009) ANZICS CORE Management Committee. The impact of early hypoglycemia and blood glucose variability on outcome in critical illness. Crit Care 13:R91
Hermanides J, Vriesendorp TM, Bosman RJ et al (2010) Glucose variability is associated with intensive care unit mortality. Crit Care Med 38:838–842
Van den Berghe G (2012) Intensive insulin therapy in the ICU—reconciling the evidence. Nat Rev Endocrinol 8:374–378
Schultz MJ, Harmsen RE, Korevaar JC et al (2012) Adoption and implementation of the original strict glycemic control guideline is feasible and safe in adult critically ill patients. Minerva Anestesiol 78:982–995
Inoue S, Egi M, Kotani J et al (2013) Accuracy of blood-glucose measurements using glucose meters and arterial blood gas analyzers in critically ill adult patients: systematic review. Crit Care 17:R48
Critchley LA, Lee A, Ho AM (2010) A critical review of the ability of continuous cardiac output monitors to measure trends in cardiac output. Anesth Analg 111:1180–1192
Van den Berghe G, Wouters P, Weekers F et al (2001) Intensive insulin therapy in critically ill patients. N Engl J Med 345:1359–1367
Umpierrez GE, Isaacs SD, Bazargan N et al (2002) Hyperglycemia: an independent marker of in-hospital mortality in patients with undiagnosed diabetes. J Clin Endocrinol Metab 87:978–982
Doenst T, Wijeysundera D, Karkouti K et al (2005) Hyperglycemia during cardiopulmonary bypass is an independent risk factor for mortality in patients undergoing cardiac surgery. J Thorac Cardiovasc Surg 130:1144
Damiano ER, El-Khatib FH, Zheng H et al (2013) A comparative effectiveness analysis of three continuous glucose monitors. Diabetes Care 36:251–259
Kapitza C, Lodwig V, Obermaier K et al (2003) Continuous glucose monitoring: reliable measurements for up to 4 days with the SCGM1 system. Diabetes Technol Ther 5:609–614
Bridges BC, Preissig CM, Maher KO et al (2010) Continuous glucose monitors prove highly accurate in critically ill children. Crit Care 14:R176
Holzinger U, Warszawska J, Kitzberger R et al (2010) Real-time continuous glucose monitoring in critically ill patients: a prospective randomized trial. Diabetes Care 33:467–472
Brunner R, Adelsmayr G, Herkner H et al (2012) Glycemic variability and glucose complexity in critically ill patients: a retrospective analysis of continuous glucose monitoring data. Crit Care 16:R17
Acknowledgements
We would like to thank the nursing staff of the surgical ICU (1 F) Department of Intensive Care Medicine, Center of Anesthesiology and Intensive Care Medicine, Hamburg-Eppendorf University Medical Center, Hamburg, Germany for helping us to perform the study.
Compliance with ethical guidelines
Conflict of interest. M. A. Punke, C. Decker, K. Wodack, D. A. Reuter and S. Kluge declare that there are no conflicts of interest. We received sensors and monitors from Medtronic free of charge.
All studies on humans described in the present manuscript were carried out with the approval of the responsible ethics committee and in accordance with national law and the Helsinki Declaration of 1975 (in its current, revised form). Informed consent was obtained from all patients included in studies.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Punke, M., Decker, C., Wodack, K. et al. Continuous glucose monitoring on the ICU using a subcutaneous sensor . Med Klin Intensivmed Notfmed 110, 360–363 (2015). https://doi.org/10.1007/s00063-014-0453-1
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00063-014-0453-1