
Abstract
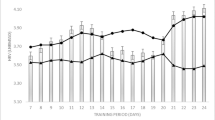
The risk of malignant arrhythmias is higher during extremely intense exercise and after its cessation. It is still unclear whether high-intensity interval exercise (HIE), an increasingly popular option in preventive and rehabilitative medicine, can lead to an impaired electrophysiological milieu, as revealed by QT interval prolongation on an electrocardiogram. This study investigated heart rate-corrected QT interval (QTc) dynamics during recovery from HIE in obese adults. In total, 13 obese males (age: 24.3 ± 4.6 years old; body mass index: 31.6 ± 4.1 kg/m2) underwent: (1) HIE: an HIE session of four 30-s all-out cycling efforts interspersed with 4‑min recovery periods; (2) REC: a recovery session 24 h after HIE; and (3) CON: a control session of no treatment. The QT interval was measured before HIE, REC, and CON, and then at 30-min intervals thereafter, for up to 3 h. QTc values were obtained using Bazett, Fridericia, Framingham, Hodges, and Rautaharju correction formulas. Acute HIE led to a significant increase in QTc for each correction (by 5–47 ms, all p < 0.05), and QTc was significantly longer during early recovery from acute exercise (HIE) compared with CON corrected with the Bazett (by 49 ms), Fridericia (by 11 ms), Hodges (by 27 ms), and Rautaharju (by 15 ms) formulas (all p < 0.05). Further, the QTc for each correction at most of the observation points in the REC trial was significantly longer (by 5–10 ms, all p < 0.05) than the corresponding value of the CON. In conclusion, in obese adults, the risk of QTc prolongation increased after brief HIE, and the risk may be sustained for more than 24 h.
Zusammenfassung
Das Risiko maligner Arrhythmien ist unter extrem intensiver Belastung und nach deren Beendigung erhöht. Noch ist unklar, ob eine Intervallbelastung hoher Intensität („high-intensity interval exercise“, HIE), eine zunehmend verbreitete Option in der Präventions- und Rehabilitationsmedizin, zu einem gestörten elektrophysiologischen Milieu führen kann, was sich durch QT-Intervall-Verlängerung im EKG zeigt. In der vorliegenden Studie wurde die herzfrequenzkorrigierte QT-Intervall(QTc)-Dynamik während der Erholung von HIE bei Adipösen untersucht. Insgesamt wurde bei 13 adipösen männlichen Probanden (Alter: 24,3 ± 4,6 Jahre; Body Mass Index: 31,6 ± 4,1 kg/m2) Folgendes durchgeführt: (1) HIE: eine HIE-Phase von vier 30-s-Phasen äußerster Anstrengung beim Radfahren, unterbrochen von 4‑min-Erholungsphasen; (2) REC: eine Erholungsphase 24 h nach HIE und (3) CON: eine Kontrollphase ohne Intervention. Das QT-Intervall wurde vor HIE, REC und CON gemessen und in 30-min-Abständen bis 3 h danach. Die QTc-Werte wurden anhand der Korrekturformeln nach Bazett, Fridericia, Framingham, Hodges und Rautaharju ermittelt. Eine akute HIE führte zum signifikanten Anstieg der QTc-Werte bei allen Korrekturen (um 5–47 ms, alle p < 0,05), und QTc war während der frühen Erholungsphase nach akuter Belastung (HIE) signifikant länger als bei CON, korrigiert mit der Formel nach Bazett (um 49 ms), Fridericia (um 11 ms), Hodges (um 27 ms) und Rautaharju (um 15 ms; alle p < 0,05). Außerdem war QTc für alle Korrekturen zu den meisten Beobachtungszeitpunkten bei REC signifikant länger (um 5–10 ms, alle p < 0,05) als die entsprechenden Werte bei CON. Das Fazit lautet, dass bei adipösen Erwachsenen das Risiko einer QTc-Verlängerung nach kurzer HIE erhöht ist und dies möglicherweise mehr als 24 h dauert.
Similar content being viewed by others

References
MacInnis MJ, Gibala MJ (2017) Physiological adaptations to interval training and the role of exercise intensity. J Physiol 595:2915–2930
Albert CM, Mittleman MA, Chae CU, Lee IM, Hennekens CH, Manson JE (2000) Triggering of sudden death from cardiac causes by vigorous exertion. N Engl J Med 343:1355–1361
Gaesser GA, Angadi SS (2011) High-intensity interval training for health and fitness: Can less be more? J Appl Physiol 111:1540–1541
Levinger I, Shaw CS, Stepto NK, Cassar S, McAinch AJ, Cheetham C, Maiorana AJ (2015) What doesn’t kill you makes you fitter: a systematic review of high-intensity interval exercise for patients with cardiovascular and metabolic diseases. Clin Med Insights Cardiol 9:53–63
Benoit SR, Mendelsohn AB, Nourjah P, Staffa JA, Graham DJ (2005) Risk factors for prolonged QTc among US adults: Third National Health and Nutrition Examination Survey. Eur J Cardiovasc Prev Rehabil 12:363–368
Omran J, Bostick BP, Chan AK, Alpert MA (2018) Obesity and ventricular repolarization: a comprehensive review. Prog Cardiovasc Dis 61:124–135
Scherr J, Schuster T, Pressler A, Roeh A, Christle J, Wolfarth B, Halle M (2012) Repolarization perturbation and hypomagnesemia after extreme exercise. Med Sci Sports Exerc 44:1637–1643
Webner D, DuPrey KM, Drezner JA, Cronholm P, Roberts WO (2012) Sudden cardiac arrest and death in United States marathons. Med Sci Sports Exerc 44:1843–1845
Gillen JB, Gibala MJ (2014) Is high-intensity interval training a time-efficient exercise strategy to improve health and fitness? Appl Physiol Nutr Metab 39:409–412
World Health Organization (2000) The Asia-Pacific perspective: redefining obesity and its treatment. Sydney: Health Communications Australia
Postema PG, Wilde AA (2014) The measurement of the QT interval. Curr Cardiol Rev 10:287–294
Vandenberk B, Vandael E, Robyns T, Vandenberghe J, Garweg C, Foulon V, Ector J, Willems R (2016) Which QT correction formulae to use for QT monitoring? J Am Heart Assoc 5:e3264
Michishita R, Ishikawa-Takata K, Yoshimura E, Mihara R, Ikenaga M, Morimura K, Takeda N, Yamada Y, Higaki Y, Tanaka H, Kiyonaga A (2015) Influence of dietary sodium and potassium intake on the heart rate corrected-QT interval in elderly subjects. J Nutr Sci Vitaminol (tokyo) 61:138–146
Mangi MA, Rehman H, Rafique M, Illovsky M (2017) Energy drinks and the risk of cardiovascular disease: a review of current literature. Cureus 9:e1322
Smetana P, Batchvarov V, Hnatkova K, Camm AJ, Malik M (2003) Circadian rhythm of the corrected QT interval: impact of different heart rate correction models. Pacing Clin Electrophysiol 26:383–386
Stewart GM, Kavanagh JJ, Koerbin G, Simmonds MJ, Sabapathy S (2014) Cardiac electrical conduction, autonomic activity and biomarker release during recovery from prolonged strenuous exercise in trained male cyclists. Eur J Appl Physiol 114:1–10
Sagie A, Larson MG, Goldberg RJ, Bengtson JR, Levy D (1992) An improved method for adjusting the QT interval for heart rate (the Framingham Heart Study). Am J Cardiol 70:797–801
Perkins SE, Jelinek HF, Al-Aubaidy HA, de Jong B (2017) Immediate and long term effects of endurance and high intensity interval exercise on linear and nonlinear heart rate variability. J Sci Med Sport 20:312–316
Cipryan L, Vala R (2015) Cardiac autonomic regulation after continuous and intermittent maximal exercise interventions. J Sports Med Phys Fitness 55:495–505
Indik JH, Pearson EC, Fried K, Woosley RL (2006) Bazett and Fridericia QT correction formulas interfere with measurement of drug-induced changes in QT interval. Heart Rhythm 3:1003–1007
De Vecchis R, Ariano C, Di Biase G, Noutsias M (2018) Acquired drug-induced long QTc: new insights coming from a retrospective study. Eur J Clin Pharmacol 74:1645–1651
Funding
The study was supported by a research grant from Macao Polytechnic Institute (RP/ESEFD-02/2012).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
J. Nie, Q. Shi, Z. Kong, C.K. Lao, H. Zhang and T.K. Tong declare that they have no competing interests.
All procedures performed in studies involving human participants or on human tissue were in accordance with the ethical standards of the institutional and/or national research committee and with the 1975 Helsinki declaration and its later amendments or comparable ethical standards. Informed consent was obtained from all individual participants included in the study.
Rights and permissions
About this article

Cite this article
Nie, J., Shi, Q., Kong, Z. et al. QTc interval prolongation during recovery from brief high-intensity intermittent exercise in obese adults. Herz 45 (Suppl 1), 67–71 (2020). https://doi.org/10.1007/s00059-019-4808-5
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00059-019-4808-5