
Abstract
Introduction
Decreasing body temperature on first follow-up visit—relative to discharge—predicts early rehospitalization in heart failure (HF). We studied whether admission-to-discharge temperature reduction was associated with increased HF rehospitalization in the ESCAPE trial.
Methods
We compared patients with or without ≥1 °C decrease in temperature from admission-to-discharge. The study endpoint was rehospitalization due to HF for up to 6 months after discharge.
Results
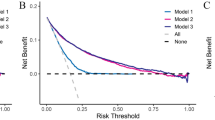
Among 354 patients (average age 57 years, 73% men) with recorded admission and discharge temperature, 22 (6.2%) had an admission-to-discharge temperature reduction ≥1 ºC. Patients with admission-to-discharge temperature reduction ≥1 ºC had higher frequency of rehospitalization for HF (68.2% vs. 44.3%, estimated odds ratio [OR] 2.697, 95% confidence interval [CI] 1.072–6.787, P = 0.029) despite a significantly higher admission temperature. On multivariate analysis, admission-to-discharge temperature reduction ≥1 ºC predicted rehospitalization for HF (OR 2.02, 95% CI 1.028–3.966, P = 0.041) after adjustment for age, BMI, baseline Na, creatinine, ejection fraction and discharge NYHA class. A standard logistic model treating temperature change as a continuous variable, and a model using a restricted cubic spline, did not demonstrate a statistically significant relationship between temperature reduction and HF rehospitalization. Subsequently, an altered logistic model was fit expressing the log odds of HF rehospitalization as a piecewise linear function of temperature decrease; this model did demonstrate statistical significance (P = 0.013) with an estimated odds ratio of 1.140 per 0.1 ºC beyond 0.5 ºC.
Conclusion
Admission-to-discharge temperature reduction ≥1 ºC is an unfavorable prognostic sign associated with future rehospitalization due to HF.
Zusammenfassung
Hintergrund
Bei Herzinsuffizienz (HF) ist eine – im Vergleich zur Temperatur bei Entlassung aus der stationären Behandlung – geringere Körpertemperatur bei der ersten Follow-up-Untersuchung ein Prädiktor für eine frühe erneute Hospitalisierung. Wir untersuchten, ob eine zum Zeitpunkt der Entlassung vergleichsweise geringere Körpertemperatur in der ESCAPE(Evaluation Study of Congestive Heart Failure and Pulmonary Artery Catheterization Effectiveness)-Studie mit einer höheren Rate an Herzinsuffizienz-bedingten Rehospitalisierungen einherging.
Methoden
Verglichen wurden Patienten mit bzw. ohne eine Verringerung der Körpertemperatur um ≥1 °C zwischen Aufnahme und Entlassung. Endpunkt der Studie war eine HF-bedingte stationäre Wiederaufnahme bis zu 8 Monaten nach Entlassung.
Ergebnisse
Von den 354 Patienten (Durchschnittsalter 57 Jahre, 73% Männer) mit dokumentierter Körpertemperatur bei Aufnahme und bei Entlassung bestand bei 22 (6,2%) eine Temperaturdifferenz von ≥‑1 ºC. Diese Patienten wiesen trotz einer signifikant höheren Temperatur bei Aufnahme eine höhere HF-bedingte Rehospitalisierungsrate auf (68,2 vs. 44,3%; geschätzte Odds Ratio, OR, 2,697; 95%-Konfidenzintervall, KI, 1,072–6,787, p = 0,029). In der multivariaten Analyse erwies sich nach Anpassung für Alter, BMI, Basis-Natrium- und -Kreatininkonzentration, Ejektionsfraktion und NYHA-Klasse bei Entlassung eine Temperaturverringerung von ≥1 ºC als prädiktiv für eine HF-bedingte Rehospitalisierung (OR 2,02; 95%-KI 1,028–3,966; p = 0,041). Ein logistisches Standardmodell mit Temperaturveränderung als einer kontinuierlichen Variablen und ein Modell unter Verwendung eines restringierten kubischen Spline zeigten keine statistisch signifikante Beziehung zwischen Temperaturabfall und HF-bedingter Rehospitalisierung. Anschließend wurde ein verändertes logistisches Modell angesetzt, in welchem die „log odds“ für eine HF-bedingte Rehospitalisierung als abschnittsweise lineare Funktion des Temperaturabfalls ausgedrückt wurde. Dieses wies eine Beziehung mit statistischer Signifikanz (p = 0,013) nach, mit einer geschätzten OR von 1,140 pro 0,1 ºC jenseits einer jeweiligen Differenz von 0,5 ºC.
Schlussfolgerung
Eine Verringerung der Körpertemperatur von ≥1 ºC zwischen Aufnahme und Entlassung ist ein ungünstiges prognostisches Zeichen und assoziiert mit einer höheren Wahrscheinlichkeit für eine HF-bedingte Rehospitalisierung.


Similar content being viewed by others

References
Hunt SA, Abraham WT, Chin MH (2009) 2009 focused update incorporated into the ACC/AHA 2005 guidelines for the diagnosis and management of heart failure in adults: a report of the American College of Cardiology Foundation/American Heart Association task force on practice guidelines. J Am Coll Cardiol 53:e1–e90
Omar HR, Guglin M (2016) Hypothermia is an independent predictor of short and intermediate term mortality in acute systolic heart failure: insights from the ESCAPE trial. Int J Cardiol 220:729–733
Nallamothu BK, Payvar S, Wang Y, Kosiborod M, Masoudi FA, Havranek EP et al (2006) Admission body temperature and mortality in elderly patients hospitalized for heart failure. J Am Coll Cardiol 47(12):2563–2564
Casscells W, Vasseghi MF, Siadaty MS, Madjid M, Siddiqui H, Lal B et al (2005) Hypothermia is a bedside predictor of imminent death in patients with congestive heart failure. Am Heart J 149(5):927–933
Payvar S, Spertus JA, Miller AB, Casscells SW, Pang PS, Zannad F et al (2013) Association of low body temperature and poor outcomes in patients admitted with worsening heart failure: a substudy of the Efficacy of Vasopressin Antagonism in Heart Failure Outcome Study with Tolvaptan (EVEREST) trial. Eur J Heart Fail 15(12):1382–1389
Ahmed A, Aboshady I, Munir SM, Gondi S, Brewer A, Gertz SD et al (2008) Decreasing body temperature predicts early rehospitalization in congestive heart failure. J Card Fail 14(6):489–496
Binanay C et al (2005) Evaluation study of congestive heart failure and pulmonary artery catheterization effectiveness: the ESCAPE trial. JAMA 294(13):1625–1633
Stone CJ, Koo CY (1985) Additive splines in statistics. In: Proceedings of the statistical computing section. American Statistical Association, Washington DC
Harrell FE Jr (2015) Regression modeling strategies: with applications to linear models, logistic and ordinal regression, and survival analysis, 2nd edn. Springer, Cham
Harrell FE Jr. (2016) rms: regression modeling strategies. R package version 4.5-0. https://cran.r-project.org/web/packages/rms/rms.pdf. Accessed: February 2017
Boulay F, Berthier F, Sisteron O, Gendreike Y, Gibelin P (1999) Seasonal variation in chronic heart failure hospitalizations and mortality in France. Circulation 100(3):280–286. https://doi.org/10.1161/01.cir.100.3.280
Stewart S, McIntyre K, Capewell S, McMurray JJ (2002) Heart failure in a cold climate. Seasonal variation in heart failure-related morbidity and mortality. J Am Coll Cardiol 39:760–766
Feldman DE, Platt R, Dery V, Kapetanakis C, Lamontagne D, Ducharme A et al (2004) Seasonal congestive heart failure mortality and hospitalization trends, Quebec 1990-1998. J Epidemiol Community Health 58(2):129–130. https://doi.org/10.1136/jech.58.2.129
Rodríguez-García JL, Paule A, Domínguez J, García-Escribano JR, Vázquez M (1999) Effects of the angiotensin II antagonist losartan on endothelin-1 and norepinephrine plasma levels during cold pressor test in patients with chronic heart failure. Int J Cardiol 70(3):293–301
Westheim A, Os I, Thaulow E, Kjeldsen SE, Eritsland J, Eide IK (1992) Haemodynamic and neurohumoral effects of cold pressor test in severe heart failure. Clin Physiol 12(1):95–106
Tei C, Horikiri Y, Park JC, Jeong JW, Chang KS, Toyama Y, Tanaka N (1995) Acute hemodynamic improvement by thermal vasodilation in congestive heart failure. Circulation 91(10):2582–2590. https://doi.org/10.1161/01.cir.91.10.2582
Gottlieb SS, Abraham W, Butler J, Forman DE, Loh E, Massie BM (2002) The prognostic importance of different definitions of worsening renal function in congestive heart failure. J Card Fail 8(3):136–141. https://doi.org/10.1054/jcaf.2002.125289
Jacobsson A, Pihl-Lindgren E, Fridlund B (2001) Malnutrition in patients suffering from chronic heart failure; the nurse’s care. Eur J Heart Fail 3(4):449–456. https://doi.org/10.1016/s1388-9842(01)00139-8
Acknowledgements
The ESCAPE trial is conducted and supported by the NHLBI in collaboration with the ESCAPE Study Investigators. This article was prepared using a limited access dataset obtained from the NHLBI and does not necessarily reflect the opinions or views of the ESCAPE trial investigators or the NHLBI.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
H.R. Omar and M. Guglin declare that they have no competing interests. R. Charnigo has been a co-investigator on two grants from AstraZeneca and has traded IBM stock and/or stock options.
This article does not contain any studies with human participants or animals performed by any of the authors.
Rights and permissions
About this article

Cite this article
Omar, H.R., Charnigo, R. & Guglin, M. Admission-to-discharge temperature reduction in decompensated heart failure is associated with rehospitalization. Herz 43, 649–655 (2018). https://doi.org/10.1007/s00059-017-4612-z
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00059-017-4612-z