
Abstract
Coronary artery disease (CAD) begins with asymptomatic atherosclerotic changes in the vessel wall. Gradual or abrupt progression of some of these early lesions eventually leads to symptomatic luminal narrowing. Coronary computed tomography angiography (CTA) allows for a minimally invasive assessment of these wall changes and of the severity of luminal narrowing, and is thus an attractive method for assessing progression/regression. However, because of the associated radiation exposure and concern about false-positive findings, CTA is not recommended as a clinical screening test. Owing to the significantly lower spatial resolution compared with invasive modalities, its application as a tool for clinical progression/regression trials is limited. Therefore, while there are extensive data from both CT coronary artery calcium scoring and CTA studies demonstrating the prognostic value of luminal stenosis as well as the extent and characteristics of plaque, data describing progression/regression are limited.
Zusammenfassung
Eine koronare Herzerkrankung beginnt mit asymptomatischen Ablagerungen in der Gefäßwand. Die graduelle oder plötzliche Progression dieser Läsionen führt schließlich zu symptomatischer Verengung des Gefäßlumens. Die koronare computertomographische Angiographie (CTA) erlaubt die minimalinvasive Untersuchung dieser Ablagerungen und Engstellen und ist theoretisch ein attraktives Verfahren für die Untersuchung der Progression/Regression. Wegen der Strahlenbelastung wird die CTA allerdings nicht als Screeninguntersuchung empfohlen, und die geringere räumliche Auflösung limitiert die Anwendung in klinischen Progressions-Regressions-Studien. Aus diesen Gründen gibt es zwar viel Erfahrung mit der koronaren CT-Untersuchung des „Kalziumscores“ (CAC) und der CTA in Bezug auf den prognostischen Wert von Engstellen sowie dem Ausmaß und den Kennzeichen von Plaque, aber es bestehen nur begrenzt Daten zur Progression/Regression.





Similar content being viewed by others

References
Taylor AJ, Cerqueira M, Hodgson JM, Mark D et al (2010) ACCF/SCCT/ACR/AHA/ASE/ASNC/ NASCI/SCAI/SCMR 2010 appropriate use criteria for cardiac computed tomography. Circulation 122:e525–e555
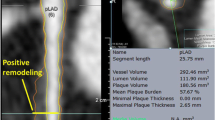
Glagov S, Weisenberg E, Zarins CK, Stankunavicius R et al (1987) Compensatory enlargement of human atherosclerotic coronary arteries. N Engl J Med 316:1371–1375
Greenland P, Bonow RO, Brundage BH, Budoff MJ et al (2007) ACCF/AHA 2007 clinical expert consensus document on coronary artery calcium scoring by computed tomography in global cardiovascular risk assessment and in evaluation of patients with chest pain: a report of the American College of Cardiology Foundation Clinical Expert Consensus Task Force. Circulation 115:402–426
Houslay ES, Cowell SJ, Prescott RJ, Reid J et al (2006) Scottish aortic stenosis and lipid lowering therapy, impact on regression trial investigators. Progressive coronary calcification despite intensive lipid-lowering treatment: a randomised controlled trial. Heart 92:1207–1212
Fischer C, Hulten E, Belur P, Smith R et al (2013) Coronary CT angiography versus intravascular ultrasound for estimation of coronary stenosis and atherosclerotic plaque burden: a meta-analysis. J Cardiovasc Comput Tomogr 7:256–266
Voros S, Rinehart S, Qian Z, Joshi P et al (2011) Coronary atherosclerosis imaging by coronary CT angiography: current status, correlation with intravascular interrogation and meta-analysis. JACC Cardiovasc Imaging 4:537–548
Springer I, Dewey M (2009) Comparison of multislice computed tomography with intravascular ultrasound for detection and characterization of coronary artery plaques: a systematic review. Eur J Radiol 71:275–282
Nair A, Kuban BD, Tuzcu EM, Schoenhagen P et al (2002) Coronary plaque classification with intravascular ultrasound radiofrequency data analysis. Circulation 106:2200–2206
Schoenhagen P, Ziada KM, Kapadia SR, Crowe TD et al (2000) Extent and direction of arterial remodeling in stable versus unstable coronary syndromes. Circulation 101:598–603
Stone GW, Maehara A, Lansky AJ, de Bruyne B et al (2011) PROSPECT investigators. A prospective natural-history study of coronary atherosclerosis. N Engl J Med 364:226–235
Achenbach S, Moselewski F, Ropers D, Ferencik M et al (2004) Detection of calcified and noncalcified coronary atherosclerotic plaque by contrast- enhanced, submillimeter multidetector spiral computed tomography: a segment-based comparison with intravascular ultrasound. Circulation 109:14–17
Leber AW, Becker A, Knez A, von Ziegler F et al (2006) Accuracy of 64-slice computed tomography to classify and quantify plaque volumes in the proximal coronary system: a comparative study using intravascular ultrasound. J Am Coll Cardiol 47:672–677
Schroeder S, Kopp AF, Baumbach A, Meisner C et al (2001) Noninvasive detection and evaluation of atherosclerotic coronary plaques with multi-slice computed tomography. J Am Coll Cardiol 37:1430–1435
Halliburton SS, Schoenhagen P, Nair A, Stillman A et al (2006) Contrast enhancement of coronary atherosclerotic plaque: a high-resolution, multidetector-row computed tomography study of pressure-perfused, human ex-vivo coronary arteries. Coron Artery Dis 17:553–560
Schoenhagen P, Tuzcu EM, Stillman AE, Moliterno DJ et al (2003) Non-invasive assessment of plaque morphology and remodeling in mildly stenotic coronary segments: comparison of 16-slice computed tomography and intravascular ultrasound. Coron Artery Dis 14:459–462
Achenbach S, Ropers D, Hoffmann U, MacNeill B et al (2004) Assessment of coronary remodeling in stenotic and nonstenotic coronary atherosclerotic lesions by multidetector spiral computed tomography. J Am Coll Cardiol 43:842–847
Imazeki T, Sato Y, Inoue F, Anazawa T et al (2004) Evaluation of coronary artery remodeling in patients with acute coronary syndrome and stable angina by multislice computed tomography. Circ J 68:1045–1050
Schoenhagen P, Baker ME (2014) Our preoccupation with ultra-low dose radiation exposure. Low contrast resolution and cardiovascular CT imaging. J Cardiovasc Comput Tomogr 8:426–428
Kitagawa T, Yamamoto H, Horiguchi J et al (2009) Characterization of non-calcified coronary plaques and identification of culprit lesions in patients with acute coronary syndrome by 64-slice computed tomography. JACC Cardiovasc Imaging 2:153–160
Motoyama S, Kondo T, Sarai M, Sugiura A et al (2007) Multislice computed tomographic characteristics of coronary lesions in acute coronary syndromes. J Am Coll Cardiol 50:319–326
Motoyama S, Sarai M, Harigaya H, Anno H et al (2009) Computed tomo- graphic angiography characteristics of atherosclerotic plaques subsequently resulting in acute coronary syndrome. J Am Coll Cardiol 54:49–57
Rinehart S, Vazquez G, Qian Z, Murrieta L et al (2011) Quantitative measurements of coronary arterial stenosis, plaque geometry, and composition are highly reproducible with a standardized coronary arterial computed tomographic approach in high-quality CT datasets. J Cardiovasc Comput Tomogr 5:35–43
Boogers MJ, Broersen A, van Velzen JE, de Graaf FR et al (2012) Automated quantification of coronary plaque with computed tomography: comparison with intravascular ultrasound using a dedicated registration algorithm for fusion-based quantification. Eur Heart J 33:1007–1016
Carrigan TP, Nair D, Schoenhagen P, Curtin RJ et al (2009) Prognostic utility of 64-slice computed tomography in patients with suspected but no documented coronary artery disease. Eur Heart J 30:362–371
Min JK, Shaw LJ, Devereux RB, Okin PM et al (2007) Prognostic value of multidetector coronary computed tomographic angiography for prediction of all-cause mortality. J Am Coll Cardiol 50:1161–1170
Chow BJ, Small G, Yam Y, Chen L, CONFIRM investigators et al (2011) Incremental prognostic value of cardiac computed tomography in coronary artery disease using CONFIRM: COroNary computed tomography angiography evaluation for clinical outcomes: an InteRnational Multicenter registry. Circ Cardiovasc Imaging 4:463–472
Hulten EA, Carbonaro S, Petrillo SP, Mitchell JD et al (2011) Prognostic value of cardiac computed tomography angiography: a systematic review and meta-analysis. J Am Coll Cardiol 57:1237–1247
Bamberg F, Sommer WH, Hoffmann V, Achenbach S et al (2011) Meta-analysis and systematic review of the long-term predictive value of assessment of coronary atherosclerosis by contrast-enhanced coronary computed tomography angiography. J Am Coll Cardiol 57:2426–2436
Ferencik M, Schlett CL, Bamberg F, Truong QA et al (2012) Comparison of traditional cardiovascular risk models and coronary atherosclerotic plaque as detected by computed tomography for prediction of acute coronary syndrome in patients with acute chest pain. Acad Emerg Med 19:934–942
Voros S, Rinehart S, Vazquez-Figueroa JG, Kalynych A et al (2014) Prospective, head-to-head comparison of quantitative coronary angiography, quantitative computed tomography angiography, and intravascular ultrasound for the prediction of hemodynamic significance in intermediate and severe lesions, using fractional flow reserve as reference standard (from the ATLANTA I and II Study). Am J Cardiol 113:23–29
Nakazato R, Shalev A, Doh JH, Koo BK et al (2013) Aggregate plaque volume by coronary computed tomography angiography is superior and incremental to luminal narrowing for diagnosis of ischemic lesions of intermediate stenosis severity. J Am Coll Cardiol 62:460–467
Park HB, Heo R, Ó Hartaigh B, Cho I et al (2015) Atherosclerotic plaque characteristics by CT angiography identify coronary lesions that cause ischemia: a direct comparison to fractional flow reserve. JACC Cardiovasc Imaging 8:1–10.
Min JK, Leipsic J, Pencina MJ, Berman DS et al (2012) Diagnostic accuracy of fractional flow reserve from anatomic CT angiography. JAMA 308:1237–1245
Tu S, Barbato E, Köszegi Z, Yang J et al (2014) Fractional flow reserve calculation from 3-dimensional quantitative coronary angiography and TIMI frame count: a fast computer model to quantify the functional significance of moderately obstructed coronary arteries. JACC Cardiovasc Interv 7:768–777
Schoenhagen P, Desai MY (2015) Computed tomography-based fractional flow reserve (FFR-CT)—an attractive concept, but still lacking proof of clinical utility. Circ J 79:300–302
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
P. Schoenhagen and F. Yan state that there are no conflicts of interest. The accompanying manuscript does not include studies on humans or animals.
Rights and permissions
About this article

Cite this article
Schoenhagen, P., Yan, F. Progression of coronary artery disease. Herz 40, 869–874 (2015). https://doi.org/10.1007/s00059-015-4344-x
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00059-015-4344-x