
Abstract
Introduction
In October 2011, a 72-year-old man was referred from a peripheral hospital with subsequent diagnosis: fungal sepsis with suspicion for endocarditis of a bioprosthetic aortic heart valve. In May 2010, a bioprosthetic aortic valve implantation (Edwards Magna) and CABG (LIMA graft on LAD) were performed.
Case
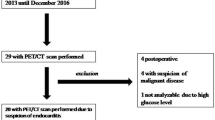
At the time of admission, the patient was in good general condition; the physical examination was unremarkable. Hemoculture detected Streptococci thermophilus and Candida parapsilosis. Neither an oscillating intracardiac mass on the valve nor an abscess could be detected in several transesophageal echocardiographies (TEEs). The F18-FDG PET-CT showed an increased tracer uptake in the area of the prosthetic aortic valve. The findings argued for a fungal endocarditis of the prosthetic aortic valve.
Heart surgeons refrained from implantation of a new prosthetic aortic valve because of the unfavorable prognosis. Therefore, highdose i.v. therapy with liposomale amphotericin B (5 mg/kg BW) and voriconazol (4 mg/kg BW twice a day) was started. A new F18-FDG PET-CT after 2 weeks showed no tracer uptake in the area of the prosthetic aortic valve. The hemoculture was also negative. The patient recovered; CRP values were within normal limits. Life-long antifungal therapy with fluconazol (400 mg/day) was recommended.
Conclusion
There are no definitive treatment recommendations for fungal endocarditis. Surgical therapy is the first choice in prosthetic valve endocarditis, which however cannot be performed in all patients. In these cases high dose and life-long medical therapy is necessary to prevent re-infection of the valve, even if (transient) deterioration of renal and liver function occurs.
Zusammenfassung
Einleitung
Im Oktober 2011 wurde ein 72-jähriger Mann mit Pilzsepsis und Verdacht auf Endokarditis mit Beteiligung der biologischen Aortenklappenprothese von einem peripheren Spital an das Uniklinikum Graz transferiert. Im Mai 2010 erhielt der Patient eine biologische Aortenklappenprothese (Edwards Magna) und einen aortokoronaren Bypass (LIMA-Graft auf LAD).
Fall
Bei der Ankunft in der klinischen Abteilung für Kardiologie präsentierte sich der Patient in einem guten Allgemeinzustand. Die physikalische Untersuchung war unauffällig. Mehrere transösophageale Echokardiographien (TEEs) ergaben weder einen Hinweis auf oszillierende Klappenauflagerungen noch auf intrakardiale Abszesse. Eine F18-FDG-PET-CT-Untersuchung detektierte einen gesteigerten Tracer-Uptake im Bereich der Aortenklappenprothese. Die vorliegenden Befunde erhärteten den Verdacht auf Pilzendokarditis mit Beteiligung der Aortenklappenprothese.
Experten der Herzchirurgie nahmen Abstand von einer Reoperation mit Neuimplantation einer Aortenklappenprothese. Man entschied sich für die Einleitung einer i.v.-Therapie mit Amphotericin B (5 mg/kg Körpergewicht) und Voriconazol (4 mg/kg KG 2-mal/Tag). In einem weiteren Kontroll-F18-FDG-PET-CT nach 2 Wochen konnte kein pathologischer Tracer-Uptake im Bereich der Aortenklappenprothese mehr nachgewiesen werden. Auch die abschließende Blutkultur war negativ, die CRP-Werte lagen im Normbereich. Eine lebenslange antifungale Therapie mit Fluconazol (400 mg/Tag) wurde empfohlen.
Fazit
Es gibt keine definitiven Therapieempfehlungen für Pilzendokarditiden. Als Mittel der Wahl gilt eine chirurgische Therapie, welche allerdings nicht in jedem Fall durchgeführt werden kann. Hier ist eine hochdosierte lebenslange medikamentöse Therapie nötig, um eine Reinfektion der Klappe zu verhindern, auch wenn (vorübergehend) eine Verschlechterung der Nieren- und Leberfunktion auftritt.

Similar content being viewed by others


References
Li JS, Sexton DJ, Mick N et al (2000) Proposed modifications to the Duke criteria for the diagnosis of infective endocarditis. Clin Infect Dis 30:633–638
Ellis ME, Al-Abdely H, Sandridge A et al (2001) Fungal endocarditis: evidence in the world literature, 1965–1995. Clin Infect Dis 32:50–62
Lye DC, Hughes A, O’Brien D, Athan E (2005) Candida glabrata prosthetic valve endocarditis treated successfully with fluconazole plus caspofungin without surgery: a case report and literature review. Eur J Clin Microbiol Infect Dis 24:753–755
Garzoni C, Nobre VA, Garbino J (2007) Candida parapsilosis endocarditis: a comparative review of the literature. Eur J Clin Microbiol Infect Dis 26:915–926
Hustinx R, Be’nard F, Alavi A (2002) Whole-body FDGPET imaging in the management of patients with cancer. Semin Nucl Med 32:35–46
Flotats A, Knuuti J, Gutberlet M et al (2011) Hybrid cardiac imaging: SPECT/CT and PET/CT. A joint position statement by the European Association of Nuclear Medicine (EANM), the European Society of Cardiac Radiology (ESCR) and the European Council of Nuclear Cardiology (ECNC). Eur J Nucl Med Mol Imaging 38:201–212
Bengel FM, Higuchi T, Javadi MS, Lautama¨ki R (2009) Cardiac positron emission tomography. J Am Coll Cardiol 54:1–15
Yen RF, Chen YC, Wu YW et al (2004) Using 18-fluoro-2-deoxyglucose positron emission tomography in detecting infectious endocarditis/endoarteritis: a preliminary report. Acad Radiol 11:316–321
Moghadam-Kia S, Nawaz A, Millar BC et al (2009) Imaging with F-FDG-PET in infective endocarditis: promising role in difficult diagnosis and treatment monitoring. Hell J Nucl Med 12:165–167
Vind SH, Hess S (2010) Possible role of PET/CT in infective endocarditis. J Nucl Cardiol 17:516–519
Bockisch A, Beyer T, Antoch G et al (2004) Positron emission tomography/computed tomography—imaging protocols, artifacts, and pitfalls. Mol Imaging Biol 6:188–199
Schouten LR, Verberne HJ, Bouma BJ et al (2008) Surgical glue for repair of the aortic root as a possible explanation for increased F-18 FDG uptake. J Nucl Cardiol 15:146–147
Conflict of interest
On behalf of all authors, the corresponding author states that there are no conflicts of interest.
Author information
Authors and Affiliations
Corresponding author
Additional information
M. Wallner and G. Steyer contributed equally to this article.
Rights and permissions
About this article
Cite this article
Wallner, M., Steyer, G., Krause, R. et al. Fungal endocarditis of a bioprosthetic aortic valve. Herz 38, 431–434 (2013). https://doi.org/10.1007/s00059-012-3715-9
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00059-012-3715-9