
Abstract
Aim
Precise bonding of attachments in aligner treatment is crucial to achieve the intended tooth movement. Thus, we evaluated five different bonding protocols for attachments used in aligner treatments with the goal of identifying the most precise protocol.
Methods
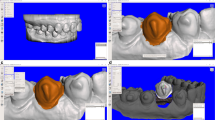
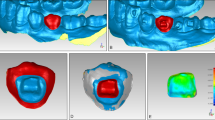
One ellipsoid and one rectangular attachment were exemplarily chosen and examined. All attachments were bonded using the same template aligner, which was produced by thermoforming. The bonding process was repeated 30 times with each protocol for statistical analysis. The protocols differed in the type of composite used (high viscous, low viscous), the additional application of a perforation in the attachment reservoir, and the use of a two-phase procedure with high viscous composite. All bonded attachments were laser scanned and compared to the attachments of a master model using a surface/surface matching algorithm to determine the precision, i.e., highest aberrations (maximum vertical distance) between the attachment of the master and results obtained from the various bonding protocols. Furthermore, the excessive amounts of composite bonded around the attachments were measured and compared.
Results
The two-phase procedure had a median aberration of 0.13 mm and a median amount of excessive composite of 7.40 mm2 (ellipsoid attachment). With the low viscous composite without a perforation in the template reservoir, similar results were achieved (median 0.13 mm) regarding the maximum vertical distance, but had an excess area of 33.50 mm2.
Conclusion
In this in vitro study, the bonding protocol influenced the precision of bonded attachments. The bonding protocol with high viscous composite without a perforation in the attachment reservoir was the most inaccurate. The use of a low viscous composite or attachments made by a two-phase procedure with high viscous composite revealed more precise results.
Zusammenfassung
Ziel
Die präzise Übertragung der geplanten Attachments auf die Zähne stellt eine Grundvoraussetzung für die Umsetzung der beabsichtigten Zahnbewegung dar. Daher evaluierten wir 5 unterschiedliche Attachment-Klebeprotokolle im Rahmen einer Alignerbehandlung mit dem Ziel, das Protokoll mit der höchsten Genauigkeit zu ermitteln.
Methode
Ein ellipsoides und ein rechteckiges Attachment wurden exemplarisch für die Untersuchungen ausgewählt und mit ein und derselben thermoplastisch hergestellten Templateschiene auf Studienmodelle geklebt. Um statistische Analysen zu ermöglichen, wurden für beide Attachments die Klebeversuche für jedes Protokoll 30-mal wiederholt. Die Protokolle unterschieden sich in der Art des verwendeten Kunststoffs (hochviskös, niedrigviskös), in der zusätzlichen Anbringung einer Perforation im Attachmentreservoir und in der Anwendung eines 2‑phasigen Vorgehens mit hochviskösem Komposit. Die Attachments wurden gescannt und mithilfe der Best-fit-Methode mit den gescannten Attachments eines Mastermodells überlagert. Um die Präzision zu bestimmen, wurde der maximale vertikale Abstand zwischen dem Attachment des Mastermodells und der Oberfläche des geklebten Attachments für jedes Protokoll gemessen. Zusätzlich wurde die Fläche des Kunststoffüberschusses um jedes Attachment erfasst und unter den Protokollen verglichen.
Ergebnisse
Bei einer mittleren Abweichung von 0,13 mm und einer durchschnittlichen Fläche an Kunststoffüberschuss von 7,40 mm2 (ellipsoides Attachment) zeigten sich die präzisesten Ergebnisse beim Klebeprotokoll mit den in einem 2‑phasigen Vorgehen mit hochviskösem Komposit hergestellten Attachments. Bezogen auf die maximale vertikale Distanz wurden ähnliche Ergebnisse beim Protokoll mit niedrigviskösem Kunststoff ohne Perforation im Attachmentreservoir ermittelt (0,13 mm im Median), es zeigte sich aber eine erhöhte durchschnittliche Kunststoffüberschussfläche von 33,50 mm2.
Schlussfolgerung
Diese In-vitro-Studie zeigt, dass das Klebeprotokoll die Präzision des Attachments beeinflusst. Das Protokoll mit hochviskösem Kunststoff ohne Perforation im Reservoir zeigte die größten Abweichungen zum Mastermodell. Bei Verwendung von fließfähigem Komposit oder von in einem 2‑phasigen Prozess mit hochviskösem Kunststoff angefertigten Attachments ergaben sich präzisere Ergebnisse.









Similar content being viewed by others

References
Abbate GM, Caria MP, Montanari P et al (2015) Periodontal health in teenagers treated with removable aligners and fixed orthodontic appliances. J Orofac Orthop 76:240–250. https://doi.org/10.1007/s00056-015-0285-5
Barreda GJ, Dzierewianko EA, Muñoz KA, Piccoli GI (2017) Surface wear of resin composites used for Invisalign® attachments. Acta Odontol Latinoam 30:90–95
Beun S, Glorieux T, Devaux J et al (2007) Characterization of nanofilled compared to universal and microfilled composites. Dent Mater 23:51–59. https://doi.org/10.1016/j.dental.2005.12.003
Böhme A, Jost-Brinkmann P‑G, Miethke R‑R (2003) Möglichkeiten der adhäsiven Befestigung von Invisalign®-Attachments. Kieferorthopädie 17:1001–1006
Dasy H, Dasy A, Asatrian G et al (2015) Effects of variable attachment shapes and aligner material on aligner retention. Angle Orthod 85:934–940. https://doi.org/10.2319/091014-637.1
Garino F, Castroflorio T, Daher S et al (2016) Effectiveness of composite attachments in controlling upper-molar movement with aligners. J Clin Orthod 50:341–347
Gomez JP, Peña FM, Martínez V et al (2015) Initial force systems during bodily tooth movement with plastic aligners and composite attachments: a three-dimensional finite element analysis. Angle Orthod 85:454–460. https://doi.org/10.2319/050714-330.1
Invisalign® Clinical Guidelines. https://learn.invisalign.com/attachments. Accessed 5 July 2018
Keilig L, Piesche K, Jäger A, Bourauel C (2006) Applications of surface–surface matching algorithms for determination of orthodontic tooth movements. Comp Methods Biomech Biomed Engin 6:353–359. https://doi.org/10.1080/10255840310001634403
Kesling HD (1945) The philosophy of the tooth positioning appliance. Am J Orthod Oral Surg 31:297–304. https://doi.org/10.1016/0096-6347(45)90101-3
Khosravi R, Cohanim B, Hujoel P et al (2017) Management of overbite with the Invisalign® appliance. Am J Orthod Dentofacial Orthop 151:691–699.e2. https://doi.org/10.1016/j.ajodo.2016.09.022
Kitasako Y, Sadr A, Burrow MF, Tagami J (2016) Thirty-six month clinical evaluation of a highly filled flowable composite for direct posterior restorations. Aust Dent J 61:366–373. https://doi.org/10.1111/adj.12387
Kuncio D (2014) Invisalign: current guidelines for effective treatment. N Y State Dent J 80:11–14
Kusai Baroudi JCR (2015) Flowable resin composites: a systematic review and clinical considerations. J Clin Diagn Res 9:ZE18–ZE24. https://doi.org/10.7860/JCDR/2015/12294.6129
Levrini L, Mangano A, Montanari P et al (2015) Periodontal health status in patients treated with the Invisalign® system and fixed orthodontic appliances: A 3 months clinical and microbiological evaluation. Eur J Dent 9:404–410. https://doi.org/10.4103/1305-7456.163218
Lu H, Tang H, Zhou T, Kang N (2018) Assessment of the periodontal health status in patients undergoing orthodontic treatment with fixed appliances and Invisalign system: a meta-analysis. Medicine 97:e248. https://doi.org/10.1097/MD.0000000000010248
McNamara JA, Kramer KL, Juenker JP (1985) Invisible retainers. J Clin Orthod 19:570–578
Ralph WJ, Jefferies JR (1984) The minimal width of the periodontal space. J Oral Rehabil 11:415–418
Ravera S, Castroflorio T, Garino F et al (2016) Maxillary molar distalization with aligners in adult patients: a multicenter retrospective study. Prog Orthod 17:12. https://doi.org/10.1186/s40510-016-0126-0
Schwarz AM (1932) Tissue changes incidental to orthodontic tooth movement. Int J Orthod 18:331–352
Shaalan OO, Abou-Auf E, El Zoghby AF (2017) Clinical evaluation of flowable resin composite versus conventional resin composite in carious and noncarious lesions: Systematic review and meta-analysis. J Conserv Dent 20:380–385. https://doi.org/10.4103/JCD.JCD_226_17
Simon M, Keilig L, Schwarze J et al (2014) Forces and moments generated by removable thermoplastic aligners: incisor torque, premolar derotation, and molar distalization. Am J Orthod Dentofacial Orthop 145:728–736. https://doi.org/10.1016/j.ajodo.2014.03.015
Simon M, Keilig L, Schwarze J et al (2014) Treatment outcome and efficacy of an aligner technique—regarding incisor torque, premolar derotation and molar distalization. BMC Oral Health 14:68. https://doi.org/10.1186/1472-6831-14-68
Skaik A, Wei XL, Abusamak I, Iddi I (2019) Effects of time and clear aligner removal frequency on the force delivered by different polyethylene terephthalate glycol-modified materials determined with thin-film pressure sensors. Am J Orthod Dentofacial Orthop 155:98–107. https://doi.org/10.1016/j.ajodo.2018.03.017
Weir T (2016) Invisalign treatment of lower incisor extraction cases. Aust Orthod J 32:82–87
White DW, Julien KC, Jacob H et al (2017) Discomfort associated with Invisalign and traditional brackets: A randomized, prospective trial. Angle Orthod 87:801–808. https://doi.org/10.2319/091416-687.1
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
J. Weckmann, S. Scharf, I. Graf, J. Schwarze, L. Keilig, C. Bourauel and B. Braumann declare that they have no competing interests.
Ethical standards
For this article no studies with human participants or animals were performed by any of the authors. All studies performed were in accordance with the ethical standards indicated in each case.
Rights and permissions
About this article

Cite this article
Weckmann, J., Scharf, S., Graf, I. et al. Influence of attachment bonding protocol on precision of the attachment in aligner treatments. J Orofac Orthop 81, 30–40 (2020). https://doi.org/10.1007/s00056-019-00204-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00056-019-00204-7
Keywords
- Orthodontic appliances, removable
- Dental bonding
- Tooth movement techniques
- In vitro techniques
- Viscosity