
Abstract
Aim
The aim of this study was to compare four different threedimensional digitalization methods on the basis of the complex anatomical surface of a cleft lip and palate plaster cast, and to ascertain their accuracy when positioning 3D landmarks.
Material and Methods
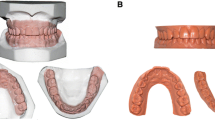
A cleft lip and palate plaster cast was digitalized with the SCAN3D® photo-optical scanner, the OPTIX 400S® laser-optical scanner, the Somatom Sensation 64® computed tomography system and the MicroScribe® MLX 3-axis articulated-arm digitizer. First, four examiners appraised by individual visual inspection the surface detail reproduction of the three non-tactile digitalization methods in comparison to the reference plaster cast. The four examiners then localized the landmarks five times at intervals of 2 weeks. This involved simply copying, or spatially tracing, the landmarks from a reference plaster cast to each model digitally reproduced by each digitalization method. Statistical analysis of the landmark distribution specific to each method was performed based on the 3D coordinates of the positioned landmarks.
Results
Visual evaluation of surface detail conformity assigned the photo-optical digitalization method an average score of 1.5, the highest subjectively-determined conformity (surpasssing computer tomographic and laser-optical methods). The tactile scanning method revealed the lowest degree of 3D landmark scatter, 0.12 mm, and at 1.01 mm the lowest maximum 3D landmark scatter; this was followed by the computer tomographic, photo-optical and laser-optical methods (in that order).
Conclusions
This study demonstrates that the landmarks’ precision and reproducibility are determined by the complexity of the reference-model surface as well as the digital surface quality and individual ability of each evaluator to capture 3D spatial relationships. The differences in the 3D-landmark scatter values and lowest maximum 3D-landmark scatter between the best and the worst methods showed minor differences. The measurement results in this study reveal that it is not the method’s precision but rather the complexity of the object analysis being planned that should determine which method is ultimately employed.
Zusammenfassung
Ziel
Das Ziel der vorliegenden Studie bestand darin, anhand der anatomisch komplexen Oberfläche eines Lippen-Kiefer-Gaumen-(LKG-)Spalten-Gipsmodells vier verschiedene räumliche Digitalisierungsverfahren einander gegenüberzustellen und deren Genauigkeit bei der 3-D-Messpunktpositionierung festzustellen.
Material und Methodik
Dazu wurde ein LKG-Spalten-Gipsmodell mit dem lichtoptischen Scanner SCAN3D®, dem laseroptischen Scanner OPTIX 400S®, dem Computertomographen Somatom Sensation 64® und dem dreiachsigen taktilen Digitalisierungsarm MicroScribe® MLX digitalisiert. Zunächst wurden durch vier Auswerter für die drei nichttaktilen Verfahren die subjektive Oberflächendetailtreue im Vergleich zum Referenz-Gipsmodell visuell beurteilt und benotet. Anschließend wurde von den vier Auswertern eine Messpunktpositionierung in fünf Durchgängen im Abstand von 2 Wochen wiederholt durchgeführt. Dabei sollten die Messpunktpositionen lediglich von einem Referenzmodell aus Gips auf das durch das entsprechende Verfahren digital reproduzierte Modell übertragen bzw. räumlich ertastet werden. Anhand der räumlichen Koordinaten der gesetzten Messpunkte erfolgte die statistische Prüfung der verfahrensspezifischen Messpunktstreuung.
Ergebnisse
Die visuelle Beurteilung der Oberflächendetailtreue bescheinigte der lichtoptischen Digitalisierungsmethode mit der Durchschnittsnote 1,5 vor dem computertomographischen und laseroptischen Verfahren die höchste subjektiv wahrgenommene Genauigkeit. Für die taktile Abtastung der Messpunkte konnte mit 0,12 mm die geringste räumliche Messpunktstreuung und mit 1,01 mm die kleinste maximale räumliche Messpunktabweichung festgestellt werden. Danach folgten das computertomographische, lichtoptische und laseroptische Verfahren.
Schlussfolgerungen
Die vorliegende Studie verdeutlicht, dass die Genauigkeit und Reproduzierbarkeit der Messpunkte nicht nur von der Komplexität der Referenzmodelloberfläche, sondern auch von der digitalen Oberflächengüte und des damit verbundenen individuellen räumlichen Erfassungsvermögens des einzelnen Auswerters bestimmt wird. Die Differenzen der Messwerte der räumlichen Messpunktabweichung und die der kleinsten maximalen räumlichen Messpunktabweichung zwischen dem besten und dem schlechtesten Verfahren zeigten nur geringe Unterschiede. Die Ergebnisse ließen den Schluss zu, dass nicht die Methodengenauigkeit, sondern die Komplexität der durchzuführenden Objektanalyse die Verfahrenswahl bestimmen sollte.
Similar content being viewed by others


References
Ayoub AF, Wray D, Moos KF, et al. A three-dimensional imaging system for archiving dental study casts: a preliminary report. Int J Adult Orthod Orthognath Surg 1997;12(1):79–84.
Badawi-Fayad J, Cabanis EA. Three-dimensional Procrustes analysis of modern human craniofacial form. Anat Rec (Hoboken). 2007;290:268–76.
Berkowitz S, Pruzansky A. Stereophotogrammetry of serial casts of cleft palate. Angle Orthod 1968;38:136–61.
Bollmann F, Dirksen D, Koslow J, et al. 3D-Koordinatenerfassung mittels computerunterstützter Profilometrie für zahnmedizinische Modellanalysen. Dtsch Zahnärztl Z 1997;52:105–8.
Braumann B, Rosenhayn SE, Bourauel C, Jäger A. Two- or three-dimensional cast analysis in patients with cleft lip palate? J Orofac Orthop 2001;62:451–65.
Braumann B, Keilig L, Bourauel C, Jäger A. Three-dimensional analysis of morphological changes in the maxilla of patients with cleft lip an palate. Cleft Palate J 2002;39:1–11.
Breukmann B, Halbauer F. Optische 3D-Koordinatenmeßtechnik. In: Breukmann B, Hrsg. Bildverarbeitung und optische Messtechnik in der industriellen Praxis: Grundlagen der 3D-Meßtechnik, Farbbild-analyse, Holographie und Interferometrie mit zahlreichen praktischen Applikationen. München: Franzis-Verlag, 1993:273.
Brief J, Behle JH, Stellzig-Eisenhauer A, Hassfeld S. Precision of landmark positioning on digitized models from patients with cleft lip and palate. Cleft Palate Craniofac J 2006;43:168–73.
Brosky ME, Major RJ, DeLong R, Hodges JS. Evaluation of dental arch reproduction using three-dimensional optical digitization. J Prosthet Dent 2003;90:434–40.
Burke PH, Beard FH. Stereophotogrammetry of the face. Amer J Orthod 1967;53:781–96.
Cattrysse E, Baeyens JP, Van Roy P, et al. Intra-articular kinematics of the upper limb joints: a six degrees of freedom study of coupled motions. Ergonomics 2005;48:1657–71.
Cha BK, Choi JI, Jost-Brinkmann PG, Jeong YM. Applications of three-dimensionally scanned models in orthodontics. Int J Comput Dent 2007;10:41–52.
Cheffins OW, Clark WAS. Close range photogrammetry applied to research in orthodontics. Photogramm Rec 1969;6:276–84.
Chen H, Lowe AA, Strauss AM, et al. Dental changes evaluated with a 3D computer-assisted model analysis after long-term tongue retaining device wear in OSA patients. Sleep Breath 2008;12:169–78.
Chen SY, Li YF, Zhang J. Vision processing for realtime 3-D data acquisition based on coded structured light. IEEE Trans Image Process 2008;17:167–76.
Commer P, Bourauel C, Maier K, Jäger A. Construction and testing of a computer-based intraoral laser scanner for determining tooth positions. Med Eng Phys 2000;22:625–35.
Coward TJ, Scott BJ, Watson RM, Richards R. A comparison between computerized tomography, magnetic resonance imaging, and laser scanning for capturing 3-dimensional data from a natural ear to aid rehabilitation. Int J Prosthodont 2006;19:92–100.
Dastane A, Vaidyanathan TK, Vaidyanathan J, et al. Development and evaluation of a new 3-D digitization and computer graphic system to study the anatomic tissue and restoration surfaces. J Oral Rehabil 1996;23:25–34.
Hayasaki H, Martins RP, Gandini LG, et al. A new way of analyzing occlusion 3 dimensionally. Am J Orthod Dentofacial Orthop. 2005 Jul;128(1):128–32.
Hayashi K, Uechi J, Lee SP, Mizoguchi I. Three-dimensional analysis of orthodontic tooth movement based on XYZ and finite helical axis systems. Eur J Orthod 2007;29:589–95.
Hense W. Nachuntersuchung kieferorthopädisch behandelter Patienten mit dem Modellmeßgerät Modellmat und dem Computerprogramm „Modell”. Bonn: Med Diss, 1984.
Hewlett ER, Orro ME, Clark GT. Accuracy testing of three-dimensional digitizing systems. Dent Mater 1992;8:49–53.
Huang BY, Durrant CJ, Johnson CW, Murray GM. A method of indirect registration of the coordinates of condylar points with a six-degree-of-freedom jaw tracker. J Neurosci Methods 2002;117:183–91.
Keß K, Kolbowski J. Computergestützte dreidimensionale Modellanalyse. Prakt Kieferorthop 1990;4:213–18.
Martensson B, Ryden H. The holodent system, a new technique for measurement and storage of dental casts. Am J Orthod Dentofacial Orthop 1992;102:113–9.
Masharawi Y, Rothschild B, Dar G, et al. Facet orientation in the thoracolumbar spine: three-dimensional anatomic and biomechanical analysis. Spine 2004;29:1755–63.
Mehl A, Gloger W, Kunzelmann KH, Hickel R. Entwicklung eines neuen optischen Oberflächenmeßgerätes zur präzisen dreidimensionalen Zahnvermessung. Dtsch Zahnärztl Z 1996;51:23.
Miras D, Sander FG. The accuracy of holograms compared to other model measurements. Fortschr Kieferorthop 1993;54:203–17.
Motohashi N, Kuroda T. A 3D computeraided design system applied to diagnosis and treatment planning in orthodontics and orthognathic surgery. Eur J Orthod 1999;21:263–74.
Oosterkamp BC, van der Meer WJ, Rutenfrans M, Dijkstra PU. Reliability of linear measurements on a virtual bilateral cleft lip and palate model. Cleft Palate Craniofac J 2006;43:519–23.
Pandya A, Siadat MR, Auner G, et al. Development and human factors analysis of neuronavigation vs. augmented reality. Stud Health Technol Inform 2004;98:291–7.
Ras F, Habets LL, van Ginkel FC, Prahl-Andersen B. Quantification of facial morphology using stereophotogrammetry — demonstration of a new concept. J Dent 1996;24:369–74.
Regensburger K, Schenk HJ, Wiemann C. Die Stereophotogrammetrie und ihre Anwendung in der stomatologischen Forschung. Zahn-, Mund- u. Kieferheilkd 1980;68:786–800.
Robertson NRE. Contour photography. Br J Orthod 1976;3:105–9.
Rydén H, Bjelkhagen H, Måtensson B. Tooth position measurements on dental casts using holographic images. Am J Orthod 1982;81: 310–3.
Sander FG. Die Verwendung der Holografie in der Kieferorthopädie für die Modellanalyse. Prakt Kieferorthop 1989;3:145–52.
Sander FG, Tochtermann H. Dreidimensionale computergestützte Modell- und Hologrammauswertung. Fortschr Kieferorthop 1991; 52:218–29.
Schenk HJ. Kieferorthopädische Modellanalyse mit Hilfe der Nahstereophotometrie. Berlin: Med Diss, 1981.
Smahel Z, Trefny P, Formanek P, et al. Three-dimensional morphology of the palate in subjects with isolated cleft palate at the stage of permanent dentition. Cleft Palate Craniofac J 2003;40:577–84.
Takasaki H. Moire topography. Appl Opt 1970;9:1457–72.
Thielke S, Serrano JG, Lepe X. A method for true coordinate three-dimensional measurement of casts using a measuring microscope. J Prosthet Dent 1998;80:506–10.
Trefny P, Smahel Z, Formanek P, Peterka M. Three-dimensional analysis of maxillary dental casts using Fourier transform profilometry: precision and reliability of the measurement. Cleft Palate Craniofac J 2004;41:20–6.
Van der Linden FP, Boersma H, Zelders T, et al. Three-dimensional analysis of dental casts by means of the Optocom. J Dent Res 1972;51:1100.
Wakabayashi K, Sohmura T, Nakamura T, et al. New evaluation method by microfocus radiograph CT for 3D assessment of internal adaptation of all-ceramic crowns. Dent Mater J 2005;24:362–7.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Boldt, F., Weinzierl, C., Hertrich, K. et al. Comparison of the Spatial Landmark Scatter of Various 3D Digitalization Methods. J Orofac Orthop 70, 247–263 (2009). https://doi.org/10.1007/s00056-009-0902-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00056-009-0902-2