
Abstract
Background
Total thyroidectomy is well accepted as initial surgery for papillary thyroid cancer (PTC), but the extent of the thyroidectomy remains a matter of controversy. This study was designed to investigate the long-term clinical outcome of PTC patients who had undergone thyroid lobectomy and to elucidate the indications of lobectomy as initial surgery.
Methods
The cases of 1,088 PTC patients who underwent thyroid lobectomy with curative intent at Ito Hospital between 1986 and 1995 were analyzed retrospectively in this study. None of the patients had received postoperative radioactive iodine (RAI) ablation therapy. The median follow-up period was 17.6 years. All clinical outcomes, including recurrence and death as a result of PTC or other reasons, were evaluated. To establish the indications for lobectomy as initial surgery for PTC, the potential risk factors, such as age, sex, primary tumor size, extrathyroidal invasion, and clinical lymph node metastasis at the time of the initial surgery, were assessed statistically for associations with recurrence and disease-related death.
Results
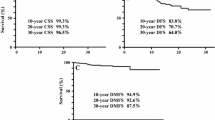
The remnant-thyroid recurrence-free survival (RT-RFS) rate, the regional- lymph-node recurrence-free survival (L-RFS) rate, and the distant-recurrence-free survival (D-RFS) rate as of 25 years after surgery were 93.5, 90.6, and 93.6%, respectively. The cause-specific survival (CSS) rate at 25 years was 95.2%. Univariate and multivariate analyses showed that none of the factors assessed were significantly associated with the RT-RFS rate. Tumor size, clinical lymph node metastasis, and extrathyroidal invasion were significantly associated with the L-RFS rate. The D-RFS and CSS rates were both significantly lower in the group of patients who were aged 45 years old or older, the group whose tumors were larger than 40 mm, and the group with extrathyroidal invasion. Based on the above findings, we classified the patients into four groups according to age <45 or ≥45 years, tumor size ≤40 or >40 mm, whether clinical lymph node metastasis was present, and whether extrathyroidal invasion was present. None of the patients without any of these four risk factors died of PTC. On the other hand, 22 patients who died of PTC were positive for one or more of these four factors.
Conclusions
The long-term clinical outcome of the PTC patients who had been treated by lobectomy without RAI ablation was excellent. Based on the above results, we concluded that lobectomy is a valid alternative to total thyroidectomy for the treatment of PTC patients who are younger than aged 45 years, whose tumor diameter is 40 mm or less, and who do not have clinical lymph node metastasis or extrathyroidal invasion.





Similar content being viewed by others

References
American Cancer Society (2011) Cancer Facts & Figures 2011. Available via www.cancer.org/acs/groups/content/@epidemiologysurveilance/documents/document/acspc-029771.pdf. Accessed 8 Feb 2012
Takami H, Ito Y, Okamoto T et al (2011) Therapeutic strategy for differentiated thyroid carcinoma in Japan based on a newly established guideline managed by Japanese society of thyroid surgeons and Japanese association of endocrine surgeons. World J Surg 35:111–121. doi:10.1007/s00268-010-0832-6
Hundahl SA, Fleming ID, Fremgen AM et al (1998) A national cancer data base report on 53,856 cases of thyroid carcinoma treated in the U.S., 1985–1995. Cancer 83:2638–2648
Shigematsu N, Takami H, Ito N et al (2005) Nation survey on the treatment policy for well-differentiated thyroid cancer. Results of a questionnaire distributed at the 37th meeting of the Japanese Society of Thyroid Surgery. Endocr J 52:479–491
Cooper DS, Doherty GM, Haugen BR et al (2009) Revised American thyroid association management guidelines for patients with thyroid nodules and differentiated thyroid cancer. Thyroid 19:1167–1213
National Comprehensive Cancer Network (2010) NCCN clinical practice guidelines in oncology. Thyroid carcinoma, vol 1. Available via http://www.nccn.org/professionals/physician_gls/pdf/thyroid.pdf. Accessed 1 Jan 2013
Cobin RH, Gharib H, Bergman DA, Thyroid Carcinoma Task Force et al (2001) AACE/AAES medical/surgical guidelines for clinical practice: management of thyroid carcinoma. American Association of Clinical Endocrinologists. American college of endocrinology. Endocr Pract 7:202–220
British Thyroid Association (2007) Guidelines for the management of thyroid cancer, 2nd edn. Available via www.british-thyroid-assiciation.org/news/Docs/Thyroid_cancer_guidelines_2007.pdf. Accessed 8 Feb 2012
DeLellis RA, Lloyd RV, Heitz PU et al (2004) WHO classification of tumours, pathology and genetics of tumours of endocrine organs. IRAC Press, Lyon, pp 73–76
Hay ID, Bergstralh EJ, Goellner JR et al (1993) Predicting outcome in papillary thyroid carcinoma: development of a reliable prognostic scoring system in a cohort of 1,779 patients surgically treated at one institution during 1940 through 1989. Surgery 114:1050–1058
Hay ID, Grant CS, Taylor WF et al (1987) Ipsilateral lobectomy versus bilateral lobar resection in papillary thyroid carcinoma: a retrospective analysis of surgical outcome using a novel prognostic scoring system. Surgery 102:1088–1094
Cady B, Rossi R (1988) An expanded view of risk-group definition in differentiated thyroid carcinoma. Surgery 104:947–953
Shaha JP, Loree TR, Dharker D et al (1992) Prognostic factors in differentiated carcinoma of the thyroid gland. Am J Surg 164:658–661
Simpson WJ, McKinney SE, Carruthers JS et al (1987) Papillary and follicular thyroid cancer: prognostic factors in 1,578 patients. Am J Med 83:479–488
Kingma G, van den Bergen HA, de Vries JE (1991) Prognostic scoring systems in differentiated thyroid carcinoma: which is the best? Neth J Surg 43:63–66
Peto R, Pike MC, Armitage P et al (1977) Design and analysis of randomized clinical trials requiring prolonged observation of each patients. II. Analysis and examples. Br J Cancer 35:1–39
Cox DR (1972) Regression models and life tables. J Roy Stat B 34:187–204
Cooper DS, Doherty GM, Haugen BR et al (2009) Revised American thyroid association management guidelines for patients with thyroid nodules and differentiated thyroid cancer. Thyroid 19:1167–1214
Gharib H, Papini E, Valcavi R, AACE/AME Task Force on Thyroid Nodules et al (2006) American association of clinical endocrinologists and associazione medici endocrinologi medical guidelines for clinical practice for the diagnosis and management of thyroid nodules. Endocr Pract 12:63–102
Pacini F, Schlumberger M, Dralle H, European Thyroid Cancer Taskforce et al (2006) European consensus for the management of patients with differentiated thyroid carcinoma of the follicular epithelium. Eur J Endocrinol 154:787–803
Sherman SI, Angelos P, Ball DW, National Comprehensive Cancer Network Thyroid Carcinoma Panel et al (2007) Thyroid Carcinoma. J Natl Compr Canc Netw 5:568–621
Bilimoria KY, Bentrem DJ, Ko CY et al (2007) Extent of surgery affects survival for papillary thyroid cancer. Ann Surg 246:375–381 discussion 381–384
Wanebo H, Coburn M, Teates D et al (1998) Total thyroidectomy does not enhance disease control or survival even in high-risk patients with differentiated thyroid cancer. Ann Surg 227:912–921
Haigh PI, Urbach DR, Rotstein LE et al (2005) Extent of thyroidectomy is not a major determinant of survival in low- or high-risk papillary thyroid cancer. Ann Surg Oncol 12:81–89
Mazzaferri EL, Young RL, Oertel JE et al (1977) Papillary thyroid carcinoma: the impact of therapy in 576 patients. Medicine (Baltimore) 56:171–196
Russel WO, Ibanz ML, Clark RL et al (1963) Thyroid carcinoma: classification, intraglandular dissemination and clinicopathological study based upon whole organ sections of 80 glands. Cancer 16:1425–1460
Clark RL, White EC, Russel WO (1959) Total thyroidectomy for cancer of the thyroid: significance of intraglandular dissemination. Ann Surg 149:858–866
Black BM, Kirk TA, Woolner LB (1960) Multicentricity of papillary adenocarcinoma of the thyroid: influence on treatment. J Clin Endocrinol Metab 20:130–135
Samaan NA, Maheshwari YK, Nader S et al (1983) Impact of therapy for differentiated carcinoma of the thyroid: an analysis of 706 cases. J Clin Endocrinol Metab 56:1131–1138
Grant CS, Hay ID, Gough IR et al (1988) Local recurrence in papillary thyroid carcinoma: is extent of surgical resection important? Surgery 104:954–962
Tollefsen H, Shaha J, Huvos A (1972) Papillary carcinoma of the thyroid. Am J Surg 124:468–472
Cohn KH, Bäckdahl M, Forsslund G et al (1984) Biologic considerations and operative strategy in papillary thyroid carcinoma: arguments against the routine performance of total thyroidectomy. Surgery 96:957–971
Rose RG, Kelsy MP, Russel WO et al (1963) Follow-up study of thyroid cancer treated by unilateral lobectomy. Am J Surg 106:494–500
Vickery AL, Wang CA, Walker AM (1987) Treatment of intrathyroidal papillary carcinoma of the thyroid. Cancer 60:2587–2595
Mazzaferri EL, Jhiang SM (1994) Long-term impact of initial surgical and medical therapy on papillary and follicular thyroid cancer. Am J Med 97:418–428
Mazzaferri EL (1999) An overview of the management of papillary and follicular thyroid carcinoma. Thyroid 9:421–427
Schvartz C, Bonnetain F, Dabakuyo S et al (2012) Impact on overall survival of radioactive iodine in low-risk differentiated thyroid cancer patients. J Clin Endocrinol Metab 97:1526–1535
Gepalakrishna N, Morris LGT, Tuttle RM et al (2011) Rising incidence of second cancers in patients with low-risk (T1N0) thyroid cancer who receive radioactive iodine therapy. Cancer 117:4439–4446
Ito Y, Ichihara K, Masuoka H et al (2010) Establishment of an intraoperative staging system (iStage) by improving UICC TNM classification system for papillary thyroid carcinoma. World J Surg 34:2570–2580. doi:10.1007/s00268-010-0710-2
Sugitani I, Kasai N, Fujimoto Y et al (2004) A novel classification system for patients with PTC: addition of the new variables of large (3 cm or greater) nodal metastases and reclassification during the follow-up period. Surgery 135:139–148
Acknowledgments
The authors acknowledge the contribution that Dr. Kunihiko Ito, who passed away in November 2012, made to the present study. Dr. Ito had been the attending physician of most of the patients included in the study and had participated in the planning and execution of this study.
Conflict of interest
The authors have no conflict of interests to declare.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Matsuzu, K., Sugino, K., Masudo, K. et al. Thyroid Lobectomy for Papillary Thyroid Cancer: Long-term Follow-up Study of 1,088 Cases. World J Surg 38, 68–79 (2014). https://doi.org/10.1007/s00268-013-2224-1
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00268-013-2224-1