
Summary
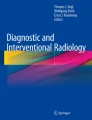
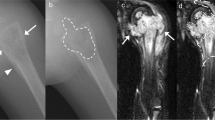
Chronic lymphoplasmacellular osteomyelitis may occur in children, adolescents and adults, but has not been found in newborns or babies either in our series or in the literature. Symptoms suggesting an acute disease like fever are uncommon, but a primary chronic course with symptomatic and asymptomatic periods is typical. Pain and swelling are the main symptoms; painless masses are rare. In children and adolescents the clavicle and metaphyseal regions of long bones are typical sites of chronic abacterial osteomyelitis. In adults the clavicles or the first two ribs are mainly affected with synovitis of the adjacent joints, but the long bones are rarely involved. Laboratory findings are non-specific but important for the differential diagnosis. The sedimentation rate and c-reactive protein might be elevated. The X-ray examination shows osteolytic, sclerotic or mixed bony changes and, in case of a diaphyseal involvement, onionskinlike periosteal bone formation may be present, suggesting a malignant process. In late stages sclerotic bone formations may be seen as a rest. Uni- or multifocal lesions can be detected by bonescan, as can asymptomatic lesions. Magnetic resonance imaging shows gross signal intensity differences both in the bone and perifocal soft tissue and involvement of the synovium with gadolinium DPTA enhancement in T1-weighted images. In early stages of the disease granulocytes, microabscesses and new bone formations might suggest bacterial osteomyelitis that cannot be differentiated by histology. In intermediate phases lymphocytic and plasmacellular infiltrates are found, whereas in late phases sclerotic bone formations and fibrosis of the bone marrow are seen histologically. In chronic lymphoplasmacellular osteomyelitis, all clinical, radiological and histological findings, as well as negative bacteriological cultures, are mandatory and will allow a definitive diagnosis to be made. The disease may be uni- or multifocal, and new bone lesions may occur over time, as well as skin manifestations, which can be found years before or after bone involvement. The association with dermatological diseases and/or synovitis led to the acronym SAPHO syndrome (synovitis, acne, pustulosis, hyperostosis, osteomyelitis). For the treatment non-steroidal anti-inflammatory drugs are effective for pain relief, reduction of swelling and dysfunction. Antibiotics have been used in several series and are not effective. Major surgery is not recommended even for recurrences, and the prognosis for growth and function is excellent in the long term despite recurrences over several years.
Zusammenfassung
Die lymphoplasmazelluläre Osteomyelitis kann im Kindes-, Jugend- und Erwachsenenalter auftreten; Erkrankungen von Säuglingen sind dagegen weder in der Literatur berichtet, noch von uns beobachtet worden. Fieber und akute Krankheitszeichen sind selten, ein primär chronischer Verlauf mit symptomatischen und asymptomatischen Phasen ist typisch. Die Hauptsymptome sind Schmerz und Schwellung, schmerzlose Schwellungen werden seltener beobachtet. Im Kindes- und Jugendalter sind besonders die Klavikula und Metaphysen der Röhrenknochen befallen. Bei Erwachsenen finden sich ganz überwiegend Osteomyelitiden der Klavikula, der ersten beiden Rippen, Synovialitiden der angrenzenden Gelenke und selten ein Befall von Extremitätenknochen. Die Laborparameter sind unspezifisch, die Blutsenkungsgeschwindigkeit und das C-reaktive Protein können mäßig erhöht sein. Das Röntgenbild zeigt meist osteolytische, gelegentlich sklerotische, häufig aber gemischte Knochenstrukturveränderungen und bei diaphysärem Befall eine zwiebelschalenartige Periostreaktion, in späteren Krankheitsphasen schließlich eine Hyperostose. In der Knochenszintigraphie findet sich regelmäßig eine Nuklidmehranreicherung und es können weitere Knochenherde, auch asymptomatische nachgewiesen werden. Die Kernspintomographie zeigt meist ausgedehnte Signalveränderungen im Knochenmark, Weichteilreaktionen und oft Begleitsynovialitiden der benachbarten Gelenke. Richtungsweisend und obligat für die Diagnose sind neben den klinischen und radiologischen Befunden die Histologie sowie bakteriologische, mikroskopische und kulturelle Untersuchungen von Abstrichen und Gewebeproben. Abhängig von den Krankheitsphasen können segmentkernige Granulozyten und Mikroabszesse in akuten Phasen nachweisbar und von einer akuten bakteriellen Osteomyelitis nicht abgrenzbar sein. In der intermediären Phase finden sich ganz überwiegend Lymphozyten und Plasmazellen und schließlich in der Spätphase sklerotische Knochentrabekel und eine Knochenmarkfibrose mit nur noch vereinzelten Lymphozyten und Plasmazellen. Die Erkrankung kann mono- oder polyostotisch auftreten, es können auch im Verlauf der Erkrankung neue Knochenherde auftreten. Eine Assoziation mit Dermatosen und/oder einer Synovialitis hat zu dem Akronym SAPHO-Syndrom geführt (Synovialitis, Akne, Pustolosis, Hyperostosis, Osteomyelitis). Für diese Krankheiten sind der chronische Verlauf, der histologische Befund und der negative Erregernachweis sowie die typischen radiologischen Befunde diagnostisch richtungsweisend. Eine gute therapeutische Wirksamkeit haben nicht-steroidale Antiphlogistika, sie führen zur Schmerzreduktion, Abschwellung und erlauben eine Normalisierung der Funktion. Ausgedehnte Knochenresektionen sind in der Regel nicht indiziert. Die Prognose ist bei uni- wie bei multilokulärem Befall gut, auch wenn über Jahre Rezidive möglich sind.
Similar content being viewed by others

Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Krauspe, R., Girschick, H. & Huppertz, H. Lymphoplasmacellular osteomyelitis. Orthopäde 26, 894–901 (1997). https://doi.org/10.1007/PL00003339
Published:
Issue Date:
DOI: https://doi.org/10.1007/PL00003339