
Summary
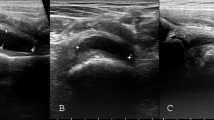
The efficiency of ultrasound was tested in septic arthritis. A total of 259 children with hip pain, septic arthritis (n = 14), transient synovitis (n = 120), juvenile rheumatoid arthritis (n = 12), Legg-Calvé-Perthes disease (n = 92) and slipped capital femoral epiphysis (n = 21) were examined by ultrasound. By using the standard planes described by the DEGUM, it is possible to analyze the joint capsule, the surface of the femoral head and the periarticular structures. In cases with synovitis or joint effusion, capsular distention can be diagnosed by ultrasound. This distention is typical in septic arthritis, transient synovitis, juvenile rheumatoid arthritis, and in the onset phase of Perthes disease. Because capsular distention and osseous abnormalities in the various diseases are similar differentiation is not possible. Therefore, ultrasound cannot distinguish between septic and non-specific arthritis; capsular distention is a non-specific ultrasound sign. Immediate diagnostic puncture is necessary if septic arthritis is suspected (possible by ultrasound control). In cases with both capsular distention and osseous abnormalities, ultrasound usually allows differentiation between slipped capital femoral epiphysis/Perthes disease and septic/non-specific arthritis.
Zusammenfassung
Die Aussagefähigkeit der Sonographie bei der bakteriellen Koxitis wurde überprüft. 259 Kinder mit Hüftschmerzen, bakterieller Koxitis (n = 14), Coxitis fugax (n = 120), juvenile rheumatoide Arthritis (n = 12), Morbus Perthes (n = 92) und Epiphyseolysis capitis femoris (n = 21) wurden sonographisch untersucht. Im Ultraschallbild können in den Standardschnittebenen der DEGUM die Gelenkkapsel, die Hüftkopfoberfläche sowie die periartikulären Strukturen beurteilt werden. Eine intraartikuläre Raumforderung (Synovialitis, Erguß) kann sonographisch als Gelenkkapseldistension erfaßt werden. Diese Kapselabhebung wurde bei der bakteriellen Koxitis, der Coxitis fugax, der juvenilen rheumatoiden Koxitis und im Frühstadium des Morbus Perthes sonographisch nachgewiesen. Da die Gelenkkapseldistension bei den einzelnen Erkrankungen keine signifikanten Unterschiede aufweist, ist aufgrund des Sonogramms beim Vorliegen einer Kapseldistension ohne knöcherne Veränderungen eine Differenzierung dieser Erkrankungen nicht möglich. Eine bakterielle Koxitis kann somit von Koxitiden anderer Genese sonographisch nicht sicher abgegrenzt werden; die Kapseldistension gilt als ein unspezifisches sonographisches Zeichen. Bei klinischem Verdacht auf eine bakterielle Koxitis ist eine unverzügliche diagnostische Punktion ggf. unter sonographischer Kontrolle erforderlich. Aufgrund zusätzlicher knöcherner Veränderungen neben der Kapseldistension lassen sich sonographisch die Epiphyseolysis capitis femoris und der Morbus Perthes im Kondensations- und Fragmentationsstadium sowohl von der bakteriellen Koxitis als auch von Koxitiden anderer Genese unterscheiden.
Similar content being viewed by others


Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Konermann, W., Gruber, G. Differential diagnosis of septic hip arthritis in childhood by ultrasound examination. Orthopäde 26, 830–837 (1997). https://doi.org/10.1007/PL00003332
Published:
Issue Date:
DOI: https://doi.org/10.1007/PL00003332