
Abstract
Objectives
The purposes of this study are to a) determine the extent to which individual and neighbourhood-level socio-economic indicators broadly reflect the social conditions associated with assault injuries within an urban Canadian city, b) examine the significance of this relationship and c) determine if this relationship is best explained at the individual or neighbourhood scale.
Methods
Assault-related hospitalization data (2001-2006) were obtained from the British Columbia Trauma Registry (BCTR). Data from the 2001 Census were used as proxy measures of individual and neighbourhood socio-economic status (SES). A generalized hierarchical nonlinear model was used to differentiate between individual and neighbourhood effects.
Results
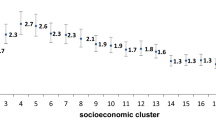
A social gradient according to individual and neighbourhood SES and frequency of assault injuries was observed for adults of all ages. After controlling for age and individual SES, probability of greater risk of assault injury among individuals living in progressively less privileged neighbourhoods remained 1.5-3 times higher than individuals living in the least deprived neighbourhoods. For adults under the age of 35, neighbourhood SES was a more statistically significant indicator of increased odds of assault injury than individual income.
Discussion
Assessing compositional and contextual variations in health outcomes provides health researchers engaged in injury surveillance a way of showing how, and for which type of people, neighbourhood environments influence the likelihood that an individual will be hospitalized due to an intentional injury. This analysis suggests that prevention efforts exclusively focused on the individual may have a limited effect in reducing the occurrence of assault-related injuries, especially among young adults.
Résumé
Objectifs
Cette étude vise à: a) déterminer s’il existe une correspondance générale entre les indicateurs socioéconomiques individuels et par quartier et les conditions sociales associées aux blessures par suite d’agressions dans une grande ville canadienne, b) examiner l’importance de cette correspondance et c) déterminer si cette correspondance s’explique le mieux à l’échelle individuelle ou du quartier.
Méthode
Les données sur les hospitalisations des victimes d’agressions (2001-2006) ont été extraites du registre des traumatismes de la Colombie-Britannique (BCTR). Les données du Recensement de 2001 ont servi de variables substitutives au statut socioéconomique (SSE) individuel et par quartier. Un modèle hiérarchique non linéaire généralisé a servi à différencier les effets individuels des effets du quartier.
Résultats
Nous avons observé, pour les adultes de tout âge, un gradient social selon le SSE individuel et du quartier et la fréquence des blessures par suite d’agressions. Compte tenu de l’âge et du SSE individuel, la probabilité d’un risque plus élevé de blessure par suite d’agression chez les personnes vivant dans des quartiers progressivement moins privilégiés demeurait de 1,5 fois à 3 fois plus élevée que chez les personnes vivant dans les quartiers les moins démunis. Chez les adultes de moins de 35 ans, le SSE du quartier était un indicateur plus significatif d’une probabilité accrue de blessure par suite d’agression que le revenu personnel.
Discussion
L’évaluation des écarts compositionnels et contextuels dans les résultats cliniques offrent aux chercheurs médicaux qui s’intéressent à la surveillance des blessures un moyen de montrer comment, et pour quels types de personnes, l’environnement du quartier influence la probabilité qu’une personne soit hospitalisée à la suite d’une agression. Cela pourrait vouloir dire que les efforts de prévention qui s’adressent exclusivement aux individus n’ont qu’un effet limité pour réduire la fréquence des blessures par suite d’agressions, surtout chez les jeunes adultes.
Similar content being viewed by others


References
Canadian Institute for Health Information. National trauma registry report: Hospital injury admissions 1998/99. Ottawa, ON: CIHI, 2001.
Cubbin C, Smith GS. Socioeconomic inequalities in injury: Critical issues in design and analysis. Annu Rev Public Health 2002;23:349–75.
Howe A, Crilly M. Deprivation and violence in the community: A perspective from a UK Accident and Emergency Department. Injury 2001;32(5):349–51.
Baker SP, O’Neill B, Ginsburg MJ, Li G. The Injury Fact Book. New York, NY: Oxford University Press, 1992.
Cubbin C, LeClere FB, Smith GS. Socioeconomic status and injury mortality: Individual and neighbourhood determinants. J Epidemiol Community Health 2000;54:517–24.
Reading R, Langford IH, Haynes R, Lovett A. Accidents to preschool children: Comparing family and neighbourhood risk factors. Soc Sci Med 1999;48:321–30.
Simpson K, Janssen I, Craig WM, Pickett W. Multilevel analysis of associations between socioeconomic status and injury among Canadian adolescents. J Epidemiol Community Health 2005;59:1072–77.
Sampson RJ, Raudenbush SW, Earls F. Neighborhoods and violent crime: A multilevel study of collective efficacy. Science 1997;277:918–24.
Wright J, Kariya A. Aetiology of assault with respect to alcohol, unemployment and social deprivation: A Scottish accident and emergency department case-control study. Injury 1997;28(5-6):369–72.
Diez-Roux A, Nieto F, Muntaner C, Tyroler HA, Comstock GW, et al. Neighborhood environments and coronary heart disease: A multilevel analysis. Am J Epidemiol 1997;146:48–63.
Diez-Roux AV. Multilevel analysis in public health research. Annu Rev Public Health 2000;21:171–92.
Macintyre S, Ellaway A, Cummins S. Place effects on health: How can we conceptualise, operationalise and measure them? Soc Sci Med 2002;55:125–39.
Bell N, Schuurman N, Oliver LN, Hayes MV. Towards the construction of place-specific measures of deprivation: A case study from the Vancouver metropolitan area. The Canadian Geographer 2007;51(4):444–61.
Oliver LN, Hayes MV. Neighbourhood socio-economic status and the prevalence of overweight Canadian children and youth. Can J Public Health 2005;96(6):415–20.
Merlo J. Multilevel analytical approaches in social epidemiology: Measures of health variation compared with traditional measures of association. J Epidemiol Community Health 2003;57:550–52.
Winkleby MA, Cubbin C. Influence of individual and neighbourhood socio-economic status on mortality among black, Mexican-American, and white women and men in the United States. J Epidemiol Community Health 2003;57(6):444–52.
Yen IH, Kaplan GA. Neighborhood social environment and risk of death: Multilevel evidence from the Alameda County Study. Am J Epidemiol 1999;149(10):898–907.
Cubbin C, Winkleby MA. Protective and harmful effects of neighborhood-level deprivation on individual-level health knowledge, behavior changes, and risk of coronary heart disease. Am J Epidemiol 2005;162(6):559–68.
Durkin M, Davidson L, Kuhn L, O’Connor P, Barlow B. Low-income neighborhoods and the risk of severe pediatric injury: A small-area analysis in northern Manhattan. Am J Public Health 1994;84(4):587–92.
Subramanian SV. The relevance of multilevel statistical methods for identifying causal neighborhood effects. Soc Sci Med 2004;58:1961–67.
Bryk AS, Raudenbush SW. Hierarchical Linear Models: Applications and Data Analysis Methods. Thousand Oaks, CA: Sage Publications, 2002.
Paterson L, Goldstein H. New statistical methods for analyzing social structures: An introduction to multilevel models. Br Educ Res J 1992;17:387–93.
Duncan C, Jones K, Moon G. Context, composition and heterogeneity: Using multilevel models in health research. Soc Sci Med 1998;46(1):97–117.
Mason WM. Comment. J Educ Behav Statistics 1995;20:221–27.
Kawachi I, Kennedy BP. The relationship of income inequality to mortality: Does the choice of indicator matter? Soc Sci Med 1997;45(7):1121–27.
Government of British Columbia. Police and Crime: Summary Statistics. Victoria, BC: Ministry of Public Safety and Solicitor General, 2006.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Bell, N., Schuurman, N. & Hameed, S.M. A Multilevel Analysis of the Socio-spatial Pattern of Assault Injuries in Greater Vancouver, British Columbia. Can J Public Health 100, 73–77 (2009). https://doi.org/10.1007/BF03405498
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/BF03405498