
Abstract
Objective
To identify factors that predict initiation of mammography and adherence with biennial screening among Canadian women aged 50–69 years.
Methods
Using data from a longitudinal panel of Canadian women interviewed in the National Population Health Survey (NPHS) in 1994/95 and 2 and 4 years later, we estimated the relative risks (RR) of mammography initiation and adherence according to socio-demographic, health and lifestyle characteristics.
Results
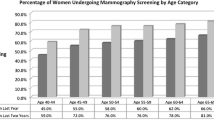
Among 505 women with no history of mammography use at baseline, 23.0% and 41.4% initiated mammography by 2 and 4 years, respectively. Urban residence (RR=2.85) was most strongly associated with initiation by 2 years; younger age (50–54) and lower education also predicted initiation by 2 years. Younger age, birthplace outside Canada, and having a recent (<2 years) blood pressure check were associated with initiation by 4 years. Among 873 women reporting a recent (<2 years) mammogram at baseline, 88.7% also reported a recent mammogram within 2 years while 73.0% reported one at both the 2- and 4-year follow-up. Being a non-smoker was the strongest predictor of maintaining adherence both at the 2- (RR=1.18) and the 4-year (RR=1.37) follow-up.
Interpretation
Previously identified underserved groups of Canadian women (e.g., those with lower educational levels or born outside of Canada) were most likely to initiate mammography. Approximately 1 in 6 women aged 50 to 69 years remained never-users during follow-up, and fewer than half reported recent mammograms at all three survey cycles, suggesting the need to reinforce regular screening participation.
Résumé
Objectif
Établir les facteurs prédictifs de la décision de subir une première mammographie et de l’adhésion à l’examen de dépistage, à tous les deux ans, chez les Canadiennes entre 50 et 69 ans.
Méthodes
À partir des données recueillies auprès d’un groupe longitudinal de Canadiennes dans le cadre de l’Enquête nationale sur la santé de la population (ENSP) de 1994–1995, puis deux et quatre ans plus tard, nous avons estimé la probabilité relative (RR) qu’une Canadienne décide de subir une première mammographie et son adhésion à cette procédure en fonction des caractéristiques socio-démographiques et des facteurs liés à la santé et au style de vie.
Résultats
En utilisant comme groupe de référence 505 femmes n’ayant jamais subi de mammographie, on constate que 23,0 % ont subi une mammographie au cours de la deuxième année et 41,4 %, de la quatrième année. On a établi un lien de corrélation très étroit entre les résidentes des zones urbaines (RR=2,85) et la décision de subir une première mammographie au cours de la deuxième année; de la même manière, l’appartenance à un groupe d’âge (de 50 à 54 ans) et un niveau de scolarité moins élevé constituaient des variables prédictives de la décision de subir une première mammographie au cours de la deuxième année. On a établi un lien de corrélation entre, d’une part, les femmes plus jeunes, nées à l’étranger et qui ont récemment (<2 ans) subi un examen de la pression artérielle et, d’autre part, la décision de subir une mammographie avant la fin de la quatrième année. En prenant comme groupe de référence 873 femmes ayant indiqué avoir dernièrement (<2 ans) subi une mammographie par rapport à l’année de référence, on constate que 88,7 % d’entre elles ont également signalé avoir subi une mammographie au cours des deux dernières années tandis que 73 % ont indiqué avoir subi un examen de suivi au cours de la deuxième et de la quatrième année. Le statut de non-fumeur représentait la première variable prédictive en importance de la décision de subir un examen de suivi au cours de la deuxième (RR=1,18) et de la quatrième année (RR=1,37).
Interprétation
Les groupes de femmes canadiennes les moins bien desservies, que l’on a déjà identifiés (p. ex., les femmes qui ont un faible niveau de scolarité et qui sont nées à l’étranger) étaient les plus susceptibles de prendre la décision de subir une mammographie. Près d’une Canadienne sur six du groupe des 50 à 69 ans n’a pas utilisé ces services durant la période de suivi et moins de la moitié d’entre elles a indiqué avoir subi des mammographies au cours des trois cycles de l’étude, suggérant ainsi la nécessité d’accroître le taux de participation à des examens de dépistage périodiques.
Similar content being viewed by others


References
National Cancer Institute of Canada. Canadian Cancer Statistics 2002. Toronto, ON, 2002.
National Cancer Institute of Canada. Canadian Cancer Statistics 2003. Toronto, ON, 2004.
Will BP, Berthelot JM, Le Petit C, Tomiak EM, Verma S, Evans, WK. Estimates of the lifetime costs of breast cancer treatment in Canada. Eur J Cancer 2000;36(6):724–35.
WHO: International Agency for Research on Cancer. Handbook for Cancer Prevention, Breast Cancer Screening. Vol. 7 edition, IARC Press, 2002.
Ballard-Barbash R, Klabunde C, Paci E, Broeders M, Coleman EA, Fracheboud J, et al. Breast cancer screening in 21 countries: Delivery of services, notification of results and outcomes ascertainment. Eur J Cancer Prev 1999;8(5):417–26.
Health Canada. Organized Breast Screening Programs in Canada: 1999 and 2000 Report. Ottawa, ON: Minister of Public Works and Government Services Canada, 2003.
World Health Organization. National Cancer Control Programmes. Policies and Managerial Guidelines. Geneva, Switzerland: WHO, 1995.
Europe Against Cancer. European Guidelines for Quality Assurance in Mammographic Screening. Luxembourg: Office for Official Publications of the European Communities, 2001.
NHSBSP. Standards for the NHS Breast Screening Programme (updated August 1998). Sheffield, England: NHSBSP Publication, 1998.
Health Canada. Report from the Evaluation Indicators Working Groups, Guidelines for Monitoring Breast Screening Program Performance. Ottawa, ON: Minister of Public Works and Government Services Canada, 2002.
Tudiver F, Fuller-Thomson E. Who has screening mammography? Results from the 1994–1995 National Population Health Survey. Can Fam Phys 1999;45:1901–7.
Zapka JG, Stoddard A, Maul L, Costanza ME. Interval adherence to mammography screening guidelines. Med Care 1991;29(8):697–707.
Phillips KA, Kerlikowske K, Baker LC, Chang SW, Brown, ML. Factors associated with women’s adherence to mammography screening guidelines. Health Serv Res 1998;33(1):29–53.
Maxwell CJ, Bancej CM, Snider J. Predictors of mammography use among Canadian women aged 50–69: Findings from the 1996/97 National Population Health Survey. CMAJ 2001;164(3):329–34.
Johnson MM, Hislop TG, Kan L, Coldman AJ, Lai A. Compliance with the screening mammography program of British Columbia: Will she return? Can J Public Health 1996;87(3):176–80.
Song L, Fletcher R. Breast cancer rescreening in low-income women. Am J Prev Med 1998;15(2):128–33.
Sabogal F, Merrill SS, Packel L. Mammography rescreening among older California women. Health Care Financ Rev 2001;22(4):63–75.
Burns RB, Freund KM, Ash A, Shwartz M, Antab L, Hall R. Who gets repeat screening mammography: The role of the physician. J Gen Intern Med 1995;10(9):520–22.
Elwood M, McNoe B, Smith T, Bandaranayake M, Doyle, TC. Once is enough—why some women do not continue to participate in a breast cancer screening programme. N Z Med J 1998;111(1066):180–83.
Fine MK, Rimer BK, Watts P. Women’s responses to the mammography experience. J Am Board Fam Pract 1993;6(6):546–55.
Snider J, Beauvais J, Levy I, Villeneuve P, Pennock J. Trends in mammography and Pap smear utilization in Canada. Chron Dis Can 1996;17(3–4):108–17.
Maxwell CJ, Kozak JF, Desjardins-Denault SD, Parboosingh J. Factors important in promoting mammography screening among Canadian women. Can J Public Health 1997;88(5):346–50.
Tambay JL, Catlin G. Sample design of the National Population Health Survey. Health Rep 1995;7(1):29–38,31–42.
Swain L, Catlin G, Beaudet, MP. The National Population Health Survey—its longitudinal nature. Health Rep 1999;10(4):69–82(ENG); 73289 (FRE).
Statistics Canada. National Population Health Survey (NPHS) Cycle 3 (1998–1999) Public Use Microdata Documentation. 2000.
Degnan D, Harris R, Ranney J, Quade D, Earp JA, Gonzalez J. Measuring the use of mammography: Two methods compared. Am J Public Health 1992;82(10):1386–88.
Gordon NP, Hiatt RA, Lampert DI. Concordance of self-reported data and medical record audit for six cancer screening procedures. J Natl Cancer Inst 1993;85(7):566–70.
Paskett ED, Tatum CM, Mack DW, Hoen H, Case LD, Velez R. Validation of self-reported breast and cervical cancer screening tests among low-income minority women. Cancer Epidemiol Biomarkers Prev 1996;5(9):721–26.
Fulton-Kehoe D, Burg MA, Lane, DS. Are selfreported dates of mammograms accurate? Public Health Rev 1992–1993;20(3–4):233–40.
Jelinski SE, Maxwell CJ, Onysko J, Bancej CM. The influence of breast self-examination on subsequent mammography participation. Am J Public Health 2005;95(3):506–11.
Bancej CM, Maxwell CJ, Snider J. Inconsistent self-reported mammography history: Findings from the National Population Health Survey longitudinal cohort. BMC Health Serv Res 2004;4(1):32.
Robbins AS, Chao SY, Fonseca, VP. What’s the relative risk? A method to directly estimate risk ratios in cohort studies of common outcomes. Ann Epidemiol 2002;12(7):452–54.
Partin MR, Slater, JS. Promoting repeat mammography use: Insights from a systematic needs assessment. Health Educ Behav 2003;30(1):97–112.
Marshall G. A comparative study of re-attenders and non-re-attenders for second triennial National Breast Screening Programme appointments. J Public Health Med 1994;16(1):79–86.
McBride CM, Curry SJ, Taplin S, Anderman C, Grothaus L. Exploring environmental barriers to participation in mammography screening in an HMO. Cancer Epidemiol Biomarkers Prev 1993;2(6):599–605.
Messina CR, Kabat GC, Lane, DS. Perceptions of risk factors for breast cancer and attitudes toward mammography among women who are current, ex- and non-smokers. Women Health 2002;36(3):65–82.
Simces Z. Community Development Pilot Projects. BC Cancer Agency Care and Research, 2002.
Cancer Care Ontario. Resource kit for providers/outreach workers who promote screening among Chinese women over 50. 2004.
Willow Breast Cancer Support and Resource Services. Responding to diversity, Phase I (1999) and Phase II (2000): A research project of Willow Breast Cancer Support and Resource Services.
St. Stephen’s Community House Toronto. Serà que Tenho Cancer na Mama? [Educational Fotonovela for use by Portuguese women]. 2003.
Lerman C, Trock B, Rimer BK, Boyce A, Jepson C, Engstrom, PF. Psychological and behavioral implications of abnormal mammograms. Ann Intern Med 1991;114(8):657–61.
Rimer BK, Trock B, Engstrom PF, Lerman C, King E. Why do some women get regular mammograms? Am J Prev Med 1991;7(2):69–74.
Urban N, Taplin SH, Taylor VM, Peacock S, Anderson G, Conrad D, et al. Community organization to promote breast cancer screening among women ages 50–75. Prev Med 1995;24(5):477–84.
Orton M, Fitzpatrick R, Fuller A, Mant D, Mlynek C, Thorogood M. Factors affecting women’s response to an invitation to attend for a second breast cancer screening examination. Br J Gen Pract 1991;41(349):320–22.
Zapka JG, Bigelow C, Hurley T, Ford LD, Egelhofer J, Cloud WM, et al. Mammography use among socio-demographically diverse women: The accuracy of self-report. Am J Public Health 1996;86(7):1016–21.
King ES, Rimer BK, Trock B, Balshem A, Engstrom P. How valid are mammography selfreports? Am J Public Health 1990;80(11):1386–88.
Suarez L, Goldman DA, Weiss, NS. Validity of Pap smear and mammogram self-reports in a low-income Hispanic population. Am J Prev Med 1995;11(2):94–98.
Warnecke RB, Sudman S, Johnson TP, O’Rourke D, Davis AM, Jobe, JB. Cognitive aspects of recalling and reporting health-related events: Papanicolaou smears, Clinical breast examinations, and mammograms. Am J Epidemiol 1997;146(11):982–92.
McGovern PG, Lurie N, Margolis KL, Slater JS. Accuracy of self-report of mammography and Pap smear in a low-income urban population. Am J Prev Med 1998;14(3):201–8.
Newell SA, Girgis A, Sanson-Fisher RW, Savolainen, NJ. The accuracy of self-reported health behaviors and risk factors relating to cancer and cardiovascular disease in the general population: A critical review. Am J Prev Med 1999;17(3):211–29.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Bancej, C.M., Maxwell, C.J., Onysko, J. et al. Mammography Utilization in Canadian Women Aged 50 to 69. Can J Public Health 96, 364–368 (2005). https://doi.org/10.1007/BF03404034
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/BF03404034