
Abstract
This research project was conducted in the Ottawa-Carleton region of Ontario to provide information on reasons why students did not participate in a Grade 7 hepatitis B school immunization project, and to determine whether telephone contact increased attendance at the community catch-up clinics above that achieved by a notice sent home with the child from school. A matched comparison group design was used.
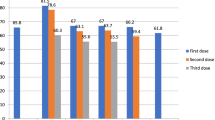
The overall uptake of the first dose of the vaccine in the region was 94% of 8,560 eligible students; 90% were immunized at the school clinic and 4% at the community catch-up clinic. About 4% of the parents refused to have their child immunized at the school or catch-up clinics. Of parents in the intervention group 198 (95%) were contacted by phone. The major reasons for non-participation at the school clinics were: (1) the child was not at school on the clinic day, or the child was sick (51%), (2) there were problems with the consent form (21%), and (3) the parents did not know of the program (10%). More students from the intervention group (72%) came for vaccination than did those of the control group (50%) (p<0.01).
Résumé
Le présent projet de recherche a été mené dans la région d’Ottawa-Carleton, en Ontario, dans le but d’expliquer pourquoi des élèves de 7e année n’ont pas participé à la séance de vaccination contre l’hépatite B tenue à l’école et de déterminer, en faisant appel à des groupes de référence appariés, si le rappel téléphonique a été un moyen plus efficace que les lettres données aux parents par l’intermédiaire des enfants pour accroître le taux de participation aux séances de vaccination dans la collectivité.
Dans la région, 94% des 8 560 élèves admissibles ont reçu la première dose du vaccin. De ce nombre, 90% se sont présentés à la séance de vaccination à l’école et 4% sont allés à la séance organisée dans la collectivité. Environ 4% des parents ont refusé que leur enfant soit immunisé lors des séances tenues à l’école ou dans la collectivité. Cent quatre-vingt-dix-huit parents du premier groupe (95%) ont été joints par téléphone. Tous les élèves n’ont pas participé à la séance de vaccination à l’école principalement parce que certains élèves étaient absents ou malades le jour de la séance (51%), les formulaires de consentement posaient des problèmes (21%) et des parents ignoraient l’existence du programme (10%). Un plus grand nombre d’élèves du premier groupe (72%) que d’élèves du second groupe (50%) (p<0,01) s’est présenté à la séance.
Similar content being viewed by others

References
D’Elage G, Carter AO. Hepatitis B infection in Canada. Epidemiology and implications for control. Can Fam Physician 1992;38:2656–66.
Alter MJ, Hadler SC, Margolis HS, et al. The changing epidemiology of hepatitis B in the United States. JAMA 1990;263:1218–22.
National Advisory Committee on Immunization. Statement on universal immunization against hepatitis B. Can Dis Wkly Rep 1991;17:165.
Infectious Disease and Immunization Committee, Canadian Paediatric Society. Hepatitis B in Canada: The case for universal immunization. Can Med Assoc J 1992;146:25–28.
Report of the Hepatitis Working Group: Can Dis Wkly Rep 1994;20:105–12.
Dobson SR, Scheifele DW, Bell A. Evaluation of a universal hepatitis B vaccination program for adolescents in British Columbia. Pediatr Res 1993;33:167A (abstract 982).
Centers for Disease Control and Prevention. Hepatitis B vaccination of adolescents — California, Louisiana and Oregon, 1992–1994. MMWR 1994;43:605–9.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Stewart, P., MacDonald, N. & Manion, I. School-based Hepatitis B Immunization Program: Follow-Up of Non-participants at First School Clinic. Can J Public Health 88, 192–196 (1997). https://doi.org/10.1007/BF03403886
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/BF03403886