
Abstract
Objective
To describe the trends over calendar period and birth cohort in lung cancer incidence by histopathology and sex, in Alberta.
Methods
Lung cancer data were extracted from the Alberta Cancer Registry for the years 1979 to 1998. Trends in age-standardized rates over calendar period and trends of age-specific rates over birth cohorts are presented. These trends are discussed in relation to historic smoking patterns.
Results
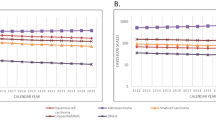
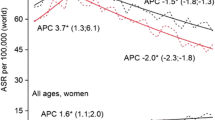
Lung cancer incidence is increasing over calendar period in females for all lung cancers and the histological types, adenocarcinoma, squamous cell, and small cell carcinoma. In males, all lung cancer incidence increases until 1988 and then decreases. Adenocarcinoma incidence in males increases over the whole time period, while squamous cell and small cell carcinoma incidence decreases. For females born before 1939, the incidence of all lung cancer and the three histological types increases over birth cohorts for all age groups. For those born after 1939, there is a slight decline. Male lung cancer incidence shows no marked increases over birth cohorts. In males born after 1929, all lung cancer and squamous cell and small cell carcinoma incidence decreases over birth cohorts for all age groups. Incidence of adenocarcinoma increases over all birth cohorts in males.
Conclusion
In Alberta, incidence of adenocarcinoma of the lung is increasing in both males and females, while squamous cell and small cell carcinoma are decreasing in males, but increasing in females. These trends may reflect changes in smoking habits.
Résumé
Objectif
Décrire les tendances de l’incidence du cancer du poumon en Alberta selon l’histopathologie et le sexe, par période du calendrier et par cohorte de naissance.
Méthode
Les données sur le cancer du poumon sont extraites du Alberta Cancer Registry (1979 à 1998). Les tendances des taux sans strate d’âges (présentées par période du calendrier) et les tendances des taux par âge (présentées par cohorte de naissance) sont analysées selon les schémas historiques du tabagisme.
Résultats
L’incidence du cancer du poumon par période du calendrier est en hausse chez les femmes pour tous les types de cancers du poumon et pour les types histologiques adénocarcinome, carcinome spinocellulaire et carcinome à petites cellules. Chez les hommes, l’incidence de tous les cancers du poumon s’accroît jusqu’en 1988 et diminue par la suite. L’incidence des adénocarcinomes chez les hommes augmente pour l’ensemble de la période, mais l’incidence des carcinomes spinocellulaires et à petites cellules diminue. Chez les femmes nées avant 1939, l’incidence par cohorte de naissance de tous les cancers du poumon et des trois types histologiques augmente pour tous les groupes d’âge. Chez les femmes nées après 1939, les taux diminuent légèrement. Globalement, l’incidence du cancer du poumon chez les hommes ne présente aucune augmentation marquée par cohorte de naissance, mais l’incidence des adénocarcinomes augmente pour toutes les cohortes de naissance, et, chez les hommes nés après 1929, l’incidence par cohorte de naissance de tous les cancers du poumon, des carcinomes spinocellulaires et des carcinomes à petites cellules diminue pour tous les groupes d’âge.
Conclusion
En Alberta, l’incidence des adénocarcinomes du poumon est en hausse tant chez les hommes que chez les femmes, tandis que l’incidence des carcinomes spinocellulaires et des carcinomes à petites cellules diminue chez les hommes, mais augmente chez les femmes. Ces tendances sont peut-être liées à l’évolution des habitudes de tabagisme.
Similar content being viewed by others

References
National Cancer Institute of Canada. Canadian Cancer Statistics 2000. Toronto, ON: NCIC, 2001.
Charloux A, Quoix E, Wolkove N, Small D, Pauli G, Kreisman H. The increasing incidence of lung adenocarcinoma: Reality or artifact? A review of the epidemiology of lung adenocarcinoma. Int J Epidemiol 1997;26(1):14–23.
Li X, Mutanen P, Hemmiki K. Gender-specific incidence trends in lung cancer by histological type in Sweden, 1958–1996. European J Cancer Prev 2001;10:227–35.
Russo A, Crosignani P, Franceschi S, Berrino F. Changes in lung cancer histological types in Varese Cancer Registry, Italy 1976–1992. European J Cancer 1997;33(10):1643–47.
Levi F, Franceschi S, La Vecchia C, Randimbison L, Te V. Lung carcinoma trends by histologic type in Vaud and Neuchatel, Switzerland, 1974–1994. Cancer 1997;79(5):906–14.
Thun M, Lally C, Flannery J, Calle E, Flanders W, Heath C. Cigarette smoking and changes in the histopathology of lung cancer. J National Cancer Institute 1997;89(21):1580–86.
Wingo P, Ries L, Giovino G, Miller D, Rosenberg H, Shopland D, et al. Annual report to the nation on the status of cancer, 1973–1996, with a special section on lung cancer and tobacco smoking. J National Cancer Institute 1999;91(8):675–90.
Stellman S, Muscat J, Thompson S, Hoffmann D, Wynder E. Risk of squamous cell carcinoma and adenocarcinoma of the lung in relation to lifetime filter cigarette smoking. Cancer 1997;80(3):382–88.
Janssen-Heijnen M, Coebergh J-M. Trends in incidence and prognosis of the histological subtypes of lung cancer in North America, Australia, New Zealand and Europe. Lung Cancer 2001;31:123–37.
Charloux A, Rossignol M, Purohit A, Small D, Wolkove N, Pauli G, et al. International differences in epidemiology of lung adenocarcinoma. Lung Cancer 1997;16:133–43.
Government of Alberta. The Alberta Cancer Programs Act 1992. Chapter C-1, Part 1.1.
WHO. International Classification of Diseases for Oncology. Geneva, Switzerland, 1976.
WHO. International Classification of Diseases for Oncology, second edition. Geneva, Switzerland, 1990.
Parkin D, Shanmugaratnam K, Sobin L, Ferlay J, Whelan S. Histological Groups for Comparative Studies. Lyon, France: IARC Technical Report No. 31, 1998.
Statistics Canada. Revised. Intercensal population and family estimates; July 1, 1971–1991. Catalogue 91–537. Ottawa, ON, 1994.
Statistics Canada. Annual demographic statistics. Demography Division, Catalogue 91-213-XPB, Annual, 1999.
Ries L, Eisner M, Kosary C, Hankey B, Miller B, Clegg L, Edwards B (Eds.). SEER Cancer Statistics Review, 1973–1999. Bethesda, MD: National Cancer Institute, 2002. Available online at: https://doi.org/seer.cancer.gov/csr/1973_1999.
Ferrence R. Sex differences in cigarette smoking in Canada, 1900-1978: A reconstructed cohort study. Can J Public Health 1988;79:160–65.
Hammond E. Smoking in relation to the death rates of one million men and women. National Cancer Institute Monograph 1966;19:127–204.
Doll R, Mill A. Mortality in relation to smoking: Ten years observation of British doctors. Br Med J 1964;1:1399–410.
The Smoking Behaviour of Canadians, 1986. Ottawa, ON: Health and Welfare Canada, 1988.
Lubin J, Blot W. Assessment of lung cancer risk factors by histologic category. JNCI 1984;73:383–89.
Wu A, Henderson B, Pike M, Yu M. Smoking and other risk factors for lung cancer in women. J Natl Cancer Inst 1985;74:747–51.
Stayner L, Wegman D. Smoking, occupation and histopathology of lung cancer: A case-control study with the use of the Third National Cancer Survey. J Natl Cancer Inst 1983;70:421–26.
Brownson R, Reif J, Keefe T, Ferguson F, Pritzl J. Risk factors for adenocarcinoma of the lung. Am J Epidemiol 1987;125:25–34.
Hoffmann D, Hoffmann I. The changing cigarette, 1950–1995. J Toxicol Environ Health 1997;50:307–64.
Wald N, Nicolaides-Bouman A (Eds.). UK Smoking Statistics, second edition. Wolfson Institute of Preventative Medicine, London: Oxford University Press, 1991.
Wynder E, Hoffmann D. Smoking and lung cancer: Scientific challenges and opportunities. Cancer Res 1994;54:5284–95.
Rickert W, Robinson J. Yields of selected toxic agents in the smoke of Canadian cigarettes, 1969 and 1978. A decade of change? Preventive Medicine 1981;10(3):353–63.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Hatcher, J., Dover, D.C. Trends in Histopathology of Lung Cancer in Alberta. Can J Public Health 94, 292–296 (2003). https://doi.org/10.1007/BF03403608
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/BF03403608