
Abstract
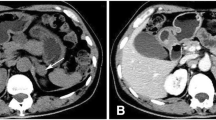
A case of unusual combination of polycystic ovaries (PCO), adrenal non-functioning adenoma and severe hirsutism in a young woman from Southern Italy is reported here. A 18-yr-old woman was referred to our Department because of oligomenhorrea, acne and severe hirsutism. During evaluation of the cause of her symptoms, PCO and small left adrenal adenoma were revealed. Although adrenal androgen excess has been shown to dysregulate the hypothalamic-pituitarygonadal axis, causing PCO-like syndrome, normal circulating androgen values were found. Androgens and cortisol levels were completely suppressed by low-dose dexamethasone test, excluding autonomous steroid secretion by the adrenal mass. Normal response of cortisol and adrenal androgens to corticotropin stimulation test permitted the exclusion of functional adrenal hyperandrogenism. Despite normal LH/FSH ratio, anovulatory cycles were revealed by persistently low progesterone values. Glucose and insulin response to oral glucose tolerance test did not differ from those of normal population. The patient showed an improvement of acne and hirsutism on therapy with estro-progestins (EP). In conclusion, despite normal pattern of serum androgens and LH/FSH ratio, this patient had anovulatory cycles and good response to the EP treatment. These findings suggest that ultrasonography evidence of PCO together with anovulatory cycles contributed to her clinical picture whereas adrenal adenoma seemed to have no relevant role. This case report underlines the need of cautious interpretation of imaging results and clinical signs of severe hirsutism, reminding one that the true cause of a medical problem may not be the most evident.
Similar content being viewed by others


References
Azziz R, Carmina E, Sawaya ME. Idiopathic hirsutism. Endocr Rev 2000, 21: 347–62.
Ferriman D, Gallway JD. Clinical assessment of body hair growth in women. J Clin Endocrinol Metab 1961, 21:1440.
Toscano V. Hirsutism: pilosebaceous unit dysregulation. Role of peripheral and glandular factors. J. Endocrinol. Invest. 1991, 14: 153–70.
Ehrmann DA, Randall BB, Rosenfield RL. Polycystic ovary syndrome as a form of functional ovarian hyperandrogenism due to dysregulation of androgen secretion. Endocr Rev 1995, 16: 322–53.
Rosenfield RL. Evidence that idiopathic functional adrenal hyperandrogenism is caused by dysregulation of adrenal steroidogenesis and that hyperinsulinemia may be involved. J Clin Endocrinol Metab 1996, 81: 878–9.
Legro RS. Polycystic ovary sindrome: the new millenium. Mol Cell Endocrinol 2001, 184: 87–93.
Dunaif A. Insulin resistance and the polycystic ovary syndrome: mechanism and implications for pathogenesis. Endocr Rev 1997, 18: 774–800.
Toscano V. Polycystic ovary sindrome: What is it? Pathogenetic enigma and therapeutic dilemma. J Endocrinol Invest 1998, 21: 546–50.
Eldar-Geva T, Hurwitz A, Vecsei P, Palti Z, Milwidsky A, Rosler A. Secondary biosynthetic defects in women with late-onset congenital adrenal hyperplasia. N Engl J Med 1990, 323: 855–63.
New MI. Diagnosis and management of congenital adrenal hyperlasia. Annu Rev Med 1998, 49: 311–28.
Valentino R, Tommaselli AP, Savastano S, Dorato M, Rossi R, Lombardi G. Different dysregulations in adrenal steroid biosynthesis as prevalent cause of hyperandrogenism in women from southern Italy. Fertil Steril 1997, 68: 236–41.
Beckers A, Parotte MC, Gaspard U, Khalife A. Hyperandrogenism: clinical aspects, investigation and treatment. Rev Med Liege 1999, 54: 274–82.
Lunde O, Djoseland O. Hirsutism caused by an androgenproducing ovarian tumor. A case of arrhenoblastoma. J Endocrinol Invest 1986, 9: 513–6.
Horton R, Lobo R. Peripheral androgens and the role of androstanediol glucuronide. Clin Endocrinol Metab 1986, 15: 293–306.
Mantero F, Terzolo M, Arnaldi G, et al. A survey on adrenal incidentaloma in Italy. J Clin Endocrinol Metab 2000, 85: 637–44.
Bertheral J, Monsler-Pudar H, Bertagna X. Adrenal Incidentalomas. Curr Opin Oncol 2002, 14: 58–63.
Erel CT, Senturk LM, Oral E, et al. Results of the ACTH stimulation test in hirsute women. J Reprod Med 1999, 44: 247–52.
Rossi R, Tauchmanova L, Luciano A, et al. Functional hyperandrogenism detected by corticotropin and GnRH-analogue stimulation tests in women affected by apparently idiopathic hirsutism. J Endocrinol Invest 2001, 24: 491–8.
Report of the Expert Committee on the Diagnosis and Classification of Diabetes Mellitus. Diabetes Care 1997, 20: 1183–1197.
Sawaya ME, Shalita AR. Androgen receptor polymorphism (CAG repeat lenghts) in androgenetic alopecia, hirsutism, and acne. J Cutan Med Surg 1998, 3: 9–15.
Miller SA, Dykes DD, Polesky HF. A simple salting-out procedure for extracting DNA from human nucleated cells. Nucleic Acids Res 1988, 16: 1215.
Hakimi JM, Schoenberg MP, Rondinelli RH, Piantadosi S, Barrack ER. Androgen receptor variants with short glutamine or glicine repeats may identify inique subpopulations of men with prostate cancer. Clin Cancer Res 1997, 3: 1599–1608.
Escobar-Morreale HF, Serrano-Gotarredona J, Garcìa- Robles R, Rancho J, Varela C. Mild adrenal and ovarian steroidogenic abnormalities in irsute women without hyperandrogenemia: does idiopathic hirsutism exist? Metabolism 1997, 46: 902–7.
Moghetti P, Castello R. New routes in the polycystic ovary syndrome labyrinth: a way out? J Endocrinol Invest 1998, 21: 648–55.
Azziz R, Bradley EL, Potter HD, et al. Adrenal androgen excess in women: lack of a role for 17-hydroxylase and 17,20-lyase dysregulation. J Clin Endocrinol Metab 1995, 80: 400–5.
Carmina E, Lobo RA. Polycysic ovaries in hirsute women with normal menses. Am J Med 2001, 111: 602–6.
Carmina E. Prevalence of idiopathic hirsutism. Eur J Endocrinol 1998, 139: 421–3.
Carmina E, Lobo A. Polycystic ovary syndrome (PCOS): arguably the most common endocrinopathy is associated with significant morbidity in women. J Clin Endocrinol Metab 1999, 84: 1897–9.
Faraj G, Di Gregorio S, Misiunas A, et al. Virilizing ovarian tumor of cell type not otherwise specified: a case report. Gynecol Endocrinol 1998, 12: 347–52.
Rossi R, Tauchmanova L, Luciano A, et al. Subclinical Cushing’s sindrome in patients with adrenal incidentaloma: clinical and biochemical features. J Clin Endocrinol Metab 2000, 85: 1440–8.
Azziz R, Bradley EL, Potter HD, et al. Adrenal androgen excess in women: lack of a role for 17-hydroxylase and 17,20- lyase disregulation. J Clin Endocrinol Metab 1995, 80: 400–5.
Rittmaster RS, Zwicker H, Thompson DL, et al. Androstanediol glucuronide production in human liver, prostte and skin. Evidence for the importance of the liver 5?-reduced androgen metabolism. J Clin Endocrinol Metab 1993, 76: 977–82.
Vottero A, Stratakis CA, Ghizzoni L, Longui CA, Karl M, Chrousos GP. Androgen receptor-mediated hypersensitivity to androgens in women with nonhyperandrogenic hirsutism: skewing of X-chromosome inactivation. J Clin Endocrinol Metab 1999, 84: 1091–5.
Calvo RM, Asuncion M, Sancho J, San Millan JL, Escobar- Morreale HF. The role of the CAG repeat polymorphism in the androgen receptor gene and of skewed X-chromosome inactivation, in the pathogenesis of hirsutism. J Clin Endocrinol Metab 2000, 85: 1735–40.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Orio, F., Palomba, S., Cascella, T. et al. Adrenal adenoma and normal androgen levels in a young woman with polycystic ovaries: A case of idiopathic hirsutism?. J Endocrinol Invest 27, 61–66 (2004). https://doi.org/10.1007/BF03350913
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/BF03350913