
Abstract
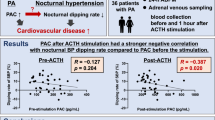
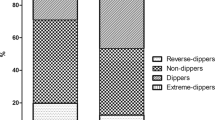
Background: The aim of the study was to evaluate diurnal blood pressure (BP) profiles in patients with primary aldosteronism and to compare them to those in subjects with essential hypertension. The effects of specific therapy on the circadian BP profiles have been studied. Materials and methods: Sixty-four patients with primary aldosteronism were included in the study. Thirty of them revealed an aldosterone-producing adenoma (APA) and 34 had idiopathic hyperaldosteronism (IHA) due to bilateral adrenal hyperplasia. Results: We did not find any significant differences in ambulatory BP monitoring (ABPM) between patients with APA and IHA. However, the circadian BP variation in the patients with primary hyperaldosteronism due to APA was preserved, while the patients with IHA showed lower nocturnal decline in comparison with patients with essential hypertension. There was a significant decline in office and ambulatory BP levels after treatment in the patients with both APA and IHA. The awake-sleep BP difference in patients with APA remained unchanged after surgical treatment, while in patients with IHA the night-time systolic and diastolic BP decline was significantly higher after spironolactone treatment. Conclusions: Primary hyperaldosteronism due to APA was associated with normal circadian BP variability and the surgical treatment led to highly significant decline in all BP parameters but had no influence on the extent of nocturnal BP variation. Spironolactone therapy restored normal nocturnal BP decline in patients with IHA. Reduction of night-time BP decline in patients with IHA is more likely to be related to the duration of the disease rather than to the aldosterone levels.
Similar content being viewed by others

References
O’Brien E. Ambulatory blood pressure monitoring in the management of hypertension. Heart 2003, 89: 571–6.
Staessen JA, Fagard RH, Lijnen PJ, Thijs L, Van Hoof R, Amery AK. Mean and range of ambulatory blood pressure in normotensive subjects from a metaanalysis of 23 studies. Am J Cardiol 1991, 67: 723–7.
Fogari R, Ambrosoli S, Corradi L, et al. 24-hour blood pressure control by once-daily administration of irbesartan assessed by ambulatory blood pressure monitoring. J Hypertens 1997, 15: 1511–8.
Pickering TG, James GD. Determinants and consequences of the diurnal rhythm of blood pressure. Am J Hypertens 1993, 6: 166S–9S.
Zakopoulos N, Stamatelopoulos S, Toumanidis S, Saridakis N, Trika C, Moulopoulos S. 24 hour blood pressure profile affects the left ventricle independently of the pressure level. A study in untreated essential hypertension. Am J Hypertens 1997, 10: 168–74.
Verdecchia P. Prognostic value of ambulatory blood pressure: current evidence and clinical implications. Hypertension 2000, 35: 844–81.
Coca A. Circadian rhythm and blood pressure control: physiological and pathophysiological factors. J Hypertens 1994, 12 (Suppl 5): S13–21
Tuck ML, Stern N, Sowers JR. Enhanced 24-hour norepinephrine and renin secretion in young patients with essential hypertension: Relation with the circadian pattern of arterialblood pressure. Am J Cardiol 1985, 55: 112–5.
Armbruster H, Vettre W, Beckerhoff R, Nussberger J, Vetter H, Siegenthaler W. Diurnal variations of plasma aldosterone in supine man: Relationship to plasma renin activity and plasma cortisol. Acta Endocrinol (Copenh) 1975, 80: 95–103.
Mancia G, Sega R, Bravi C, et al. Ambulatory blood pressure normality: results from PAMELA study. J Hypertens 1995, 13: 1377–90.
Guidelines Sub-Committee 1999 World Health Organization/ International Society of Hypertension Guidelines for the management of Hypertension. J Hypertens 1999, 17: 151–83.
Guidelines Committee. 2003 European Society of Hypertension-European Society of Cardiology guidelines for the management of arterial hypertension. J Hypertens 2003, 21: 1011–53.
Verdecchia P, Porcellati C, Schillaci G, et al. Ambulatory blood pressure. An independent predictor of prognosis of essential hypertension. Hypertension 1994, 24: 793–801.
Staessen JA, Bieniaszewski L, O’Brien E, et al. Nocturnal blood pressure fall on ambulatory monitoring in a large international database. Hypertension 1997, 29: 30–9.
Imai Y, Abe K, Sasaki S, et al. Circadian blood pressure variation in patients with renovascular hypertension or primary aldosteronism. Clin Exp Hypertens A, 1992, 14: 1141–67.
Spieker C, Barenbrock M, Rahn KH, Zidek W. Circadian blood pressure variations in endocrine disorders. Blood Pressure 1993, 2: 35–9.
Veglio F, Pinna G, Melchio R, et al. Twenty-four hour power spectral analysis by maximum entropy method of blood pressure in primary aldosteronism. Blood Pressure 1993, 2: 189–96.
Mansoor GA, White WB. Circadian blood pressure variation in hypertensive patients with primary hyperaldosteronism. Hypertension 1998, 31: 843–7.
Kimura Y, Kawamura M, Onodera S, Hiramori S. Controlled study of circadian rhythm of blood pressure in patients with aldosterone-producing adenoma compared with those with essential hypertension. J Hypertens 2000, 18: 21–5.
Penzo M, Palatini P, Rossi G P, et al. In primary aldosteronism the circadian blood pressure rhythm is similar to that in primary hypertension. Clin Exp Hypertens 1994, 16: 659–73.
Middeke M, Schrader J. Nocturnal blood pressure in normotensive subjects and those with white coat, primary and secundary hypertension. Br Med J 1994, 308: 630–2.
Uzu T, Nishimura M, Fujii T, et al. Changes in the circadian rhythm of blood pressure in primary aldosteronism in response to dietary sodium restriction and adrenalectomy. J Hypertens 1998, 16: 1745–8.
Rabbia F, Veglio F, Sibon M P, et al. Fourier analysis of circadian blood pressure profile in secondary hypertension. J Hum Hypertens 1997, 11: 295–9.
Takakuwa H, Shimizu K, Izumiya, et al. Dietary sodium restriction restores nocturnal reduction of blood pressure in patients with primary aldosteronism. Hypertens Res 2002, 25: 737–42.
Higashi Y, Oshima T, Ozono R, et al. Nocturnal decline in blood pressure is attenuated by NaCl loading in salt-sensitive patients with essential hypertension. Noninvasive 24-hour ambulatory blood pressure monitoring. Hypertension 1997, 30: 163–7.
Zelinka T, Widimsky J. Twenty-four hour blood pressure profile in subjects with different subtypes of primary aldosteronism. Physiol Res 2001, 50: 51–7.
Kem DC, Weinberger MH, Gomez-Sanchez C, et al. Circadian rhythm of plasma aldosterone concentration in patients with primary aldosteronism. J Clin Invest 1973, 52: 2272–7.
Uzu T, Kimura G. Diuretics shift circadian rhythm of blood pressure from nondipper to dipper in essential hypertension. Circulation 1999, 100: 1635–8.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Zacharieva, S., Orbetzova, M., Elenkova, A. et al. Diurnal blood pressure pattern in patients with primary aldosteronism. J Endocrinol Invest 29, 26–31 (2006). https://doi.org/10.1007/BF03349173
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/BF03349173