
Abstract
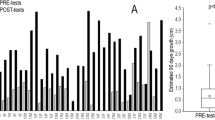
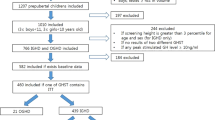
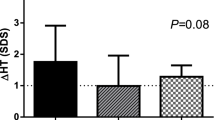
We evaluated the growth hormone (GH) response to an acute Clonidine test (0.15 mg/m2 po) in 30 normal prepubertal children (stature between the 3rd and 97th centile), in 29 short children (stature <3rd centile for age) with height velocity (HV) >10th centile and in 20 short children with HV <10th centile. The three groups had comparable chronological ages. After clonidine administration mean peak GH levels were similar in the three groups (19.4±9.8, 17.7±8.8 and 14.6±8.9 μg/l, mean±SD, respectively). By chosing 10 μg/l as the limit for a normal response we found that stimulated GH levels had a sensitivity of 50% and a specificity of 83% in identifying children with suspected GHD (short children with subnormal HV). The diagnostic accuracy was almost superimposable, for cutoff values of 10 and 12 μg/l. Eight of the 10 children with subnormal HV and a GH peak <10 μg/l had a GH peak <10 μg/l also after a second stimulation test. Six of the 29 short children with normal HV had a GH peak <10 μg/l. Only one of them had a GH peak <10 μg/l after a second stimulation test. Five of the normal children had peak GH levels <10 μg/l. These results indicate that HV is a useful variable to predict the GH response to an acute GH stimulus, since the great majority of children with a normal growth rate had a normal GH response to at least one stimulation test.
Similar content being viewed by others
References
Spiliotis B.E., August G.P., Hung W., Sonis W., Mendelson W., Bercu B.B. Growth hormone neurosecretory dysfunction: a treatable cause of short stature. JAMA 251: 2223, 1984.
Zadik Z., Chalew S.A., Raiti S., Kowarski A.A. Do short children secrete insufficient growth hormone? Pediatrics 76: 355, 1985.
Rose S.R., Ross J.L., Uriarte M., Barnes K., Cassorla F.G., Cutler G.B. The advantage of measuring stimulated as compared with spontaneous growth hormone levels in the diagnosis of growth hormone deficiency. N. Engl. J. Med. 319: 201, 1988.
Lanes R. Diagnostic limitations of spontaneous growth hormone measurements in normally growing prepubertal children. Am. J. Dis. Child. 143: 1284, 1989.
Zadik Z., Chalew S.A., Kowarski A. Assessment of growth hormone secretion in normal stature children using 24-hour integrated concentration of GH and pharmacological stimulation. J. Clin. Endocrinol. Metab. 71: 932, 1990.
Gil-Ad I., Topper E., Laron Z. Oral Clonidine as a growth hormone stimulation test. Lancet 2: 278, 1979.
Fraser N.C., Seth J., Brown N.S. Clonidine is a better test for growth hormone deficiency than insulin hypoglycaemia. Arch. Dis. Child. 58: 355, 1983.
Dattani M.T., Pringle P.J., Hindmarsh P.C., Brook C.G.D. What is a normal stimulated growth hormone concentration? J. Endocrinol. 133: 447, 1992.
Albertson-Wikland K., Rosberg S. Analyses of 24-hour growth hormone profiles in children: relation to growth. J. Clin. Endocrinol. Metab. 67: 493, 1988.
Underwood L.E., D’Ercole A.J., Van Wyk J.J. Somatomedin-C and the assessment of growth. Pediatr. Clin. North Am. 27: 771, 1980.
Lee P.D.K., Wilson D.M., Rountree L., Hinz R.L., Rosenfeld R.G. Efficacy of insulin-like growth factor I levels in predicting the response to provocative growth hormone testing. Pediatr. Res. 27: 45, 1990.
Rudman D., Kutner M.H., Chawla R.K. The short child with subnormal plasma somatomedin C. Pediatr. Res. 19: 975, 1985.
Rosenfeld R.G., Wilson D.M., Lee P.D.K., Hinz R.L. Insulin-like growth factors I and II in evaluation of growth retardation. J. Pediatr. 109: 428, 1986.
Oerter K.E., Sobel A.M., Rose S.R., Cristiano A., Malley J.D., Cutler G.B. jr., Baron J. Combining insulin-like growth factor-I and mean spontaneous nighttime growth hormone levels for the diagnosis of growth hormone deficiency. J. Clin. Endocrinol Metab. 75: 1413, 1992.
Dammacco F., Boghen M., Camanni F., Cappa M., Ferrari C., Ghigo E., Giordano G., Loche S., Minuto F., Mucci M., Müller E.E. Somatotropic function in short stature. Evaluation by integrated auxological and hormonal indices in 214 children. J. Clin. Endocrinol. Metab., 77: 68, 1993..
Brook C.G.D. Treatment of growth deficiency. Clin. Endocrinol. (Oxf.) 30: 197, 1988.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Loche, S., Cappa, M., Ghigo, E. et al. Growth hormone response to oral clonidine test in normal and short children. J Endocrinol Invest 16, 899–902 (1993). https://doi.org/10.1007/BF03348953
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/BF03348953