
Abstract
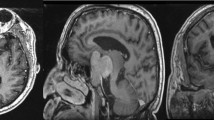
Pituitary apoplexy is a rare and underdiagnosed clinical syndrome. It results from hemorrhagic infarction of the pituitary gland. In its classical form it is characterized by acute headache, ophthalmoplegia, visual loss and pituitary insufficiency. Meningeal irritation signs, clinically indistinguishable from infectious meningitis, are considered rare and have not been reported as presenting signs. We report a 53-yr-old man who was admitted to hospital following acute headache, fever, neck stiffness and paresis of the left oculomotor and abducent nerves. A lumbar puncture revealed an increased number of polymorphs but with a sterile cerebral spinal fluid. Magnetic resonance imaging (MRI) showed an intrasellar mass with central necrosis in an enlarged sella. Endocrinological evaluation demonstrated insufficient thyroid, adrenocortical, and gonadal function. Necrosis within a chromophobe adenoma was found upon surgical decompression of the sella. After surgery anterior panhypopituitarism did not recover, while ophthalmoplegia subsided. The patient is now in good health under appropriate hormonal replacement therapy.
Similar content being viewed by others


References
Bleck T.P., Greenlee J.E. Approach to the patient with central nervous system infection. In: Mandell G.L., Bennett J.E., Dolin R. (Eds.), Principles and practice of infectious diseases. Fifth Edition. Churchill Livingstone, Philadelphia 2000, vol. 1, p.950.
Geiseler P.J., Nelson K.E., Levin S, Reddi K.T., Moses V.K. Community-acquired purulent meningitis: a review of 1316 cases during the antibiotic era. 1954-1976. Rev. Infect. Dis. 1980, 2: 725–745.
Berg L. Hypoglycorrhachia of noninfectious origin: Diffuse meningeal neoplasia. Neurology (Minn.) 1953, 3: 811–824.
Scully R.E., Mark E.J., McNeely W.F., et al. Weekly Clinicopathological Exercises. Case 15–2001. N. Engl. J. Med. 2001, 20: 1536–1541.
Cardoso E.R., Peterson E.W. Pituitary apoplexy: a review. Neurosurgery 1984, 14: 363–373.
Bailey P. Pathological report of a case of acromegaly, with special reference to the lesions in the hypophysis cerebri and in the thyroid gland; and a case of hemorrhage into the pituitary. Philadelphia Med. J. 1898, 1: 789–792.
Bleibtreu L. Ein fall von Akromegalic (Zerstorung der Hypophysis durch Blutung). Munch. Med. Wochenschr. 1905, 52: 2079–2080.
Brougham M., Heusner A.P., Adams R.D. Acute degenerative changes in adenomas of the pituitary body-with special references to pituitary apoplexy. J. Neurosurg. 1950, 7: 421–439.
Wakai S., Fukushima T., Teramoto A., Sano K. Pituitary apoplexy: its incidence and clinical signifiance. J. Neurosurg. 1981, 55: 187–193.
Vidal E., Cevallos R., Vidal J., et al. Twelve cases of pituitary apoplexy. Arch. Intern. Med. 1992, 152: 1893–1899.
Bills D.C., Meyer F. B., Laws E.R., et al. A retrospective analysis of pituitary apoplexy. Neurosurgery 1993, 33: 602–609.
Bjerre P., Lindholm J. Pituitary apoplexy with sterile meningitis. Acta Neurol. Scand. 1986, 74: 304–307.
Zervas N.T., Mendelson G. Treatment of acute haemorrhage of pituitary tumours. Lancet 1975, 1: 604–605.
Symon L., Mohanty S. Haemorrhage in pituitary tumours. Acta Neurochir. (Wien) 1982, 65: 41–49.
Rovit R.L. Fein J.M. Pituitary apoplexy. A review and reappraisal. J. Neurosurg. 1972, 37: 280–282.
Jolley F.L., Mabon R.L. Pituitary apoplexy. J. Med. Assoc. Ga. 1958, 47: 75–78.
Müller-Jensen A., Lüdecke D. Clinical aspects of spontaneous necrosis of pituitary tumors (pituitary apoplexy). J. Neurol. 1981, 224: 267–271.
Conomy J.P., Ferguson J.H., Brodkey J.S., Mitsumoto H. Spontaneous infarction in pituitary tumors: neurologic and therapeutic aspects. Neurology 1975, 25: 114–115.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Valente, M., Marroni, M., Stagni, G. et al. Acute sterile meningitis as a primary manifestation of pituitary apoplexy. J Endocrinol Invest 26, 754–757 (2003). https://doi.org/10.1007/BF03347359
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/BF03347359